On-demand webinar
Why stronger clinical handoffs matter in post-acute care
In this webinar, Optum Home and Community and Advisory Board examine how strengthening clinical handoffs can improve post-acute care outcomes.
July 8, 2026 | 2-minute read and 45-minute watch
0:02
Hello and welcome to today's webinar, Closing the Clinical Handoff Gap in Post Acute Care.
0:10
Before we get started, I'd like to review a few housekeeping details.
0:15
Today's webinar is being recorded and an online archive of today's event will be available within one to two business days.
0:24
If you have any trouble seeing the slides at any time during the presentation, please press F5 to refresh your screen on APC or Command R.
0:34
If you're using a Mac, you may ask a question at any time during the presentation by typing your question into the Q and A box located on the right side of your screen and pressing Enter.
0:47
And finally, I'd like to remind you of Ahip's antitrust statement located in the link just below the slide viewer.
0:55
We will, as always, comply with that statement.
0:58
Among other things, the antitrust statement prohibits us from discussing competitively sensitive information.
1:08
We are very fortunate to have with us today.
1:11
Miriam Schnitzer, Taub, Managing Director, Custom, Research and Sponsorship at Advisory Board and Jeff Langwyn, Senior Director, Care Transitions, Optum Home and Community.
1:28
At this time, I will turn the floor over to our speakers.
1:33
Thank you.
1:33
Welcome, everyone.
1:34
Thank you so much for joining us today.
1:37
We are really excited to be here with all of you because the topic that we are going to spend the next hour or so discussing doesn't always get the attention that it deserves.
1:48
And for many Medicare Advantage plans, we know it's quietly driving a significant share of avoidable cost and member disruption.
1:57
And so today we are focused on transitions of care, specifically thinking about when a patient is moving from acute or hospital inpatient care to post acute care.
2:09
We're going to be thinking about the clinical handoff that happens in that moment, what information is moving with the patient, what information is unfortunately not moving with the patient and where sometimes that breaks down.
2:24
And our hope today is to show that some of the things that are often measured around transitions of care, including hospital readmissions are really a downstream effect of what does or doesn't happen at that hand off moment.
2:39
Before we get too far into it, let me take a moment to introduce myself as well as Jeff, my Co presenter.
2:47
So again, my name is Miriam Schnitzer Taub.
2:49
I am a managing director of custom research at Advisory Board.
2:52
I've been a researcher at Advisory Board for over 10 years and have looked at a number of different topic areas including senior care, home based care and value based care.
3:02
And I'm excited to be Co presenting today with Jeff from Optum Home and Community Care Delivery.
3:07
So I'll turn it over to him to introduce himself as well.
3:11
Thanks, Miriam.
3:12
Good afternoon.
3:13
My name is Jeff Langland again.
3:14
I'm a Senior Director with Optum Home and Community Care delivery care transitions team.
3:20
I'm a physical therapist and a registered nurse and my work currently focused on leading educating, equipping care coordinators and post acute providers to just deliver reliable care transitions.
3:37
Great.
3:38
Let's look at the agenda for our time today at a high level.
3:42
I'm going to start by unpacking really why transitions of care from acute to post acute care are such a high risk moment in the care journey.
3:53
And then Jeff will shift into what's at stake, particularly for Medicare Advantage plans and then spend some time on really where plans can act, what are some specific opportunities to improve transitions and outcomes.
4:08
And then we'll close with some key takeaways and open it up for Q&A.
4:13
These are the three things that we want you to walk away with.
4:17
And you'll see these phrases, these insights repeated a couple of times throughout our presentation.
4:23
First, we hope that we can reframe readmissions not as the core problem, but as a symptom of something deeper that's happened in transitions of care.
4:35
2nd, we hope you walk away with a clear understanding of why this matters for MA plans specifically.
4:41
And lastly, a set of practical levers you can use to improve transitions of care, not just measure them.
4:50
So with all that housekeeping out of the way, let's jump in to really the why behind this challenge because we want to start by grounding the problem itself.
5:01
Why are these transitions of care so challenging and what are the consequences when the transitions breakdown?
5:09
So this is really about unpacking these hidden costs that don't always show up clearly in some of the metrics that are being measured.
5:16
To start answering these questions, we're going to look at really what makes these transitions so risky.
5:25
At a high level, transitions of care between acute and post acute care are challenging because two things are happening at the same time, accountability fragments at the same time, clinical and social risk peaks.
5:41
So what do I mean by that?
5:44
When I say that accountability fragments, I'm talking about how the primary accountability for a patient is shifting from one provider or organization to another.
5:55
Now this isn't bad.
5:56
It's actually an important part of a patient's care journey.
6:00
They now have different needs that can and should be met by different providers, all in service of getting them to be able to re enter their community, go back to their home as soon as possible.
6:12
But this is a change.
6:15
And that change happens as patients social risk peaks.
6:20
Patients now are adjusting to a new care facility, a new setting, a new care team, a new set of routines.
6:29
Their therapy schedule is potentially different.
6:32
Visiting hours are different.
6:34
This also means a change for their families.
6:38
As you know, they might be used to a specific routine of when they can visit their loved ones.
6:43
As a quick personal anecdote, my father a few years ago moved from acute care to post acute care and when I asked him about it, one of the things that he said was really challenging was that there was a whole new way of ordering his food at the post acute care facility that he had experienced in the hospital.
7:03
Another one of them was bad.
7:04
They both suited the facility well, but after several weeks of one way it was hard for my dad to switch to a different way and it made his first couple of days in the post acute care facility a little bit more challenging.
7:18
So compounding this, at this moment moment where patients are a bit vulnerable, their new care team may not have the most complete information about them.
7:30
And this combination drives individual and system level consequences.
7:37
Got some stats on the right side of this slide here.
7:41
But what they're pointing to is the fact that when patients have these poor transitions of care, they can be at risk for unnecessary rehospitalization.
7:51
And that results in high costs for everyone involved.
7:55
But that rehospitalization or readmission metric really only is telling part of the story.
8:02
I want to get into a little bit more about what that means.
8:05
Historically, healthcare has been really focused on reducing readmissions, particularly that 30 day hospital readmission metric.
8:14
It's incredibly important to track.
8:16
All of the efforts that have gone into reducing it have been important and worthwhile, But I would argue that readmission is a lagging indicator that something has gone wrong with the transition of care.
8:31
It just says that something went wrong, but not necessarily where or why.
8:36
So you can think of it as that visible part of the iceberg.
8:40
And for MA plans, that means that they're often managing costs after the fact instead of being able to prevent it.
8:48
So we need to look under the surface to really see what's going on.
8:54
And if we do that, what often emerges is an information gap.
9:00
Care teams at the post acute care facility are making time sensitive, important decisions with potentially incomplete or poorly contextualized information.
9:11
Now, want to be really clear, this isn't anyone's fault.
9:15
We'll talk in a few minutes about, you know, how the number of different stakeholders involved makes this hard.
9:22
But we can't ignore the challenge that this information gap provokes.
9:29
And if we only work on managing one metric, you risk overlooking the previous challenges that are driving that metric and that information gap, that information that is incomplete, backward looking, or poorly contextualized.
9:45
That information gap has broader consequences across the care ecosystem, and it impacts every stakeholder involved.
9:56
For patients and their caregivers, it can mean delayed care or even missed care entirely.
10:03
That can mean a more difficult recovery or potentially a deterioration of their health.
10:10
It also means that patients may have a harder time adjusting to their new care setting, to their new routine and disrupts their support systems, increasing their anxiety and frustration.
10:22
For post acute care providers in the middle of the slide here, they might be receiving limited or incomplete information, which can lead to uncertainty when they're making these care decisions.
10:34
And then they're in this really unfortunate position of having to make decisions without enough information that can lead to delays or escalations of complexity.
10:44
And finally, for MA plans, when members health deteriorates, it can require more complex care that can might end up becoming a rehospitalization or an Ed visit.
10:56
This ultimately drives up costs and contributes to overall total higher costs of care.
11:01
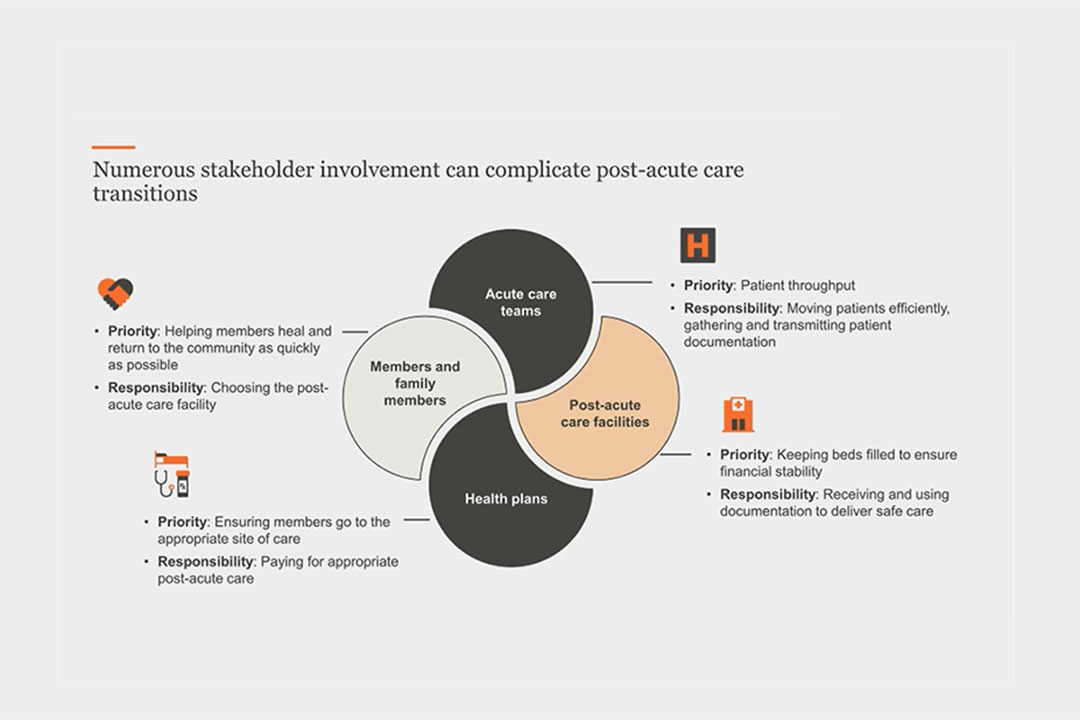
I mentioned this on the last slide, but one of the reasons this is so challenging is because there are a number of stakeholders involved in the care transition process.
11:10
So I do want to spend a moment thinking about who is involved in this process, what are their priorities and what are their responsibilities as we think about it.
11:19
So we're going to walk through this slide.
11:20
I'm going to start with the top left and then move clockwise through it.
11:24
We'll begin with members, patients and their family members.
11:29
They are making decisions during a high stress time.
11:33
Perhaps the patient has been in the acute care facility for a long time, or even if it was just a short stay, they know they can't immediately return to their home, so the priority for them is to recover or in the case of their family members, help their loved ones recover and return home as quickly as possible.
11:53
Their responsibility is to choose the facility using the best information they have at that moment.
12:00
Next, we have the acute care hospital team.
12:04
The priority here is patient throughput.
12:06
They need to ensure that patients get excellent care while in their facility and then they need to make sure that that patient can be discharged to post acute care so they can use that bed for another patient who needs their care.
12:19
Their responsibility then is to ensure that patients move efficiently while also gathering and transmitting the appropriate documentation.
12:28
Now on the bottom right, we have post acute care facilities.
12:32
They need to have an adequate number of patients to ensure their own financial stability.
12:38
So their priority then is keeping beds filled and providing that high level of care so patients can ultimately recover and move back to their home.
12:49
Their responsibility in the care transitions process is to ensure that they receive all the documentation about the patients and use it to deliver that safe, appropriate, high quality care that ultimately helps the patient return home as soon as possible.
13:03
Finally, we have health plans.
13:05
Health plans are focused on ensuring that members go to the appropriate site of care so they can receive the care that they need.
13:12
So again, ultimately they can return home and they are ultimately responsible for paying for that care.
13:19
Pulling up for a second, why did I walk through each of these?
13:22
We have 4 different stakeholder groups.
13:25
They each have the same overarching goal.
13:28
Each of them wants to be sure that that patient can return to their home as quickly as possible after receiving the care that they need to recover.
13:36
But their specific day-to-day priorities are a little bit different.
13:40
It isn't a bad thing.
13:41
It's inherent in the fact that they each serve a different role within the care ecosystem.
13:46
But what it means is that there is information, there is opportunities, sorry, for information to slip through the cracks.
13:54
And when that happens, that means there is no shared, complete view of the patient and their needs.
14:00
Each stakeholder has their own perspective, and this can create friction and ultimately make transitions of care less reliable.
14:08
This information gap ultimately makes everyone's job just a little bit more difficult.
14:14
So I hope that after this, you have started to think about this idea that poor transitions of care are really a root cause that can lead to unnecessary readmissions and re hospitalizations.
14:28
So then the question becomes, what does this mean for MA plan specifically and where can they act?
14:35
I'm going to turn it over to Jeff now to walk us through that in a little bit more detail.
14:41
Thank you, Miriam.
14:46
So now that Miriam has grounded us in the problem, we want to zoom in more on the last stakeholder she was talking about, specifically the MA plans.
14:56
Let's look at how that shows up.
14:59
So plans absorb many of the downstream cost of poor handoffs because when they're worsening outcomes as patient receives less informed care, this can lead to higher utilization and medical spend because how many plans are paid on a capitated per member per month basis.
15:17
Unplanned hospitalizations will increase medical spending.
15:21
So poor care transitions and their consequences can also lead to member dissatisfaction due to uncertainty and frustration, which can have an impact on reputation and ultimately star ratings, particularly if you keep in mind that the measures for hospital readmissions and transitions of care factor into MA plan star ratings.
15:42
Now these impacts aren't new, but what's changing is the scale of the impact.
15:48
MA penetration is rising as many of you probably know, and enrollment has been increasing with just around half of Medicare eligible individuals enrolled in a Medicare Advantage plan.
15:59
And so as the number of MA enrollees rises and they get older, it makes sense.
16:04
We're also seeing MA post acute care utilization grow just in one year.
16:09
On the slide from 2021 to 2022, MA sniff admissions increased by 12%.
16:16
So enrollment is growing, which means that understandably utilization is also increasing.
16:23
But there's one more factor and that's at the overall MA populations are becoming far more complex.
16:30
We can think specifically about the growth in the de sniffer dual eligible population.
16:35
These are individuals who are eligible for both Medicare and Medicaid and the individuals enrolled in a DECENT plan are more likely to have complex clinical profiles, higher social risk, and really fewer information resources that compensate for missing information, delayed services or unclear follow up class.
16:57
But another way poor transitions disproportionately impact these high risk MA members or DECENT members.
17:05
Going forward.
17:06
When care transitions breakdown, the consequences will be amplified across cost, quality and member experience.
17:14
So before we can decide where to intervene, we need to look at the full process and see where the information gaps occur.
17:26
An important point I hope you walk away with is that hand off failures can't be pinpointed to one single moment.
17:36
They tend to occur in multiple instances which create a compound effect.
17:41
So let's walk through the care transition process.
17:44
I know this is probably familiar to many of you, but I hope you'll be thinking about both the ideal and maybe not so ideal process and what that means for everyone involved.
17:58
Excuse me there, I think I was on the wrong slide.
18:03
There you go.
18:06
As we move through this, I want you to remember it's not about assigning blame to anyone stakeholder.
18:11
These care gaps really rarely, if ever occur intentionally or maliciously.
18:16
It's just a series of moments that when compounded have large impacts.
18:21
Let's start with discharge planning.
18:23
Now ideally, we all heard that ideally discharge planning starts at admission, but we know that too often this truly isn't the case.
18:32
Or perhaps it does start there, but something happens during a patient's acute care stay that causes the planning to be changed or abandoned.
18:41
Regardless of the reason, when discharge planning is left until later in the process, there can be delays in identifying the appropriate site of care, getting approvals and preparing documentation now, moving to the next site, site of care termination and approval.
18:58
Ideally, patients are matched to an appropriate site of care promptly and can be transferred as soon as they're clinically ready.
19:05
But perhaps identifying the correct site of care doesn't go smoothly.
19:09
This can be because the acute facility doesn't have the correct documentation to obtain the pre authorization, or the MA plan has some delays in processing the pre authorization.
19:20
Either way, the result is there can be transfer delays.
19:24
Or perhaps on the other extreme, as we've all seen, a member might be transferred too early from the acute setting, the post acute care, and wind up having poor clinical outcomes.
19:35
The next Phase I want to highlight is the handoff itself and specifically the documentation that moves along with the patient.
19:43
Ideally, providers relay all necessary information about the patient's care to the acute care facility, but also important context that serves as forward-looking guidance.
19:54
This can include the members functional trajectory, the caregiver capacity, any social instability.
20:01
This information is very important to help avoid complications.
20:05
And finally, any post discharge outreach and communications, ideally these are accurately timed to occur during the most high risk.
20:14
For the member.
20:16
But if this outreach happens too late, then MA plans have the limited ability to influence the outcomes.
20:22
With all this, it's also important to think back to the slide Miriam showed us a few minutes ago with the different stakeholders because again, we're not assigning blame, but we know that these gaps are exacerbated by misaligned incentives and trust dynamics.
20:39
Again, what we're seeing isn't a single point of failure.
20:42
It's a series of breakdowns across the process.
20:45
And that raises an important question for MA plans.
21:01
If MA fans plans don't fully control care transitions, which they don't, what is their role?
21:08
They do play a clinical role in bridging the information gap and they have clear incentive to do so.
21:14
MA plans don't own discharge decisions or select slights of care, but they do influence the environment around these decisions.
21:22
What do I mean by that?
21:23
Well, we know that plans can't select the facility for the member.
21:27
There's there's member choice involved and they don't own the moment of discharge since that's up to the medical team.
21:34
But what MA plans can do is use the data available to them to see patterns across multiple sites of care, then identify which members are at risk, which post acute partners may struggle with certain populations and then where avoidable Ed admissions or readmissions are concentrated.
21:52
They can also shape network design and performance management.
21:57
For example, they can define participation requirements.
22:01
You can ensure that members know about high performing post acute facilities and remove consistently underperforming providers from the network.
22:11
Bottom line is even with limited direct control, there are important opportunities.
22:17
So let's take a look at some of these places where plans could act.
22:26
A quick recap.
22:27
So far we've talked about why care transitions are a challenge and where the gaps can occur.
22:33
And we've introduced this idea of an information gap that we're losing critical information when patients move from one site of care to another.
22:41
So let's talk about some of the opportunities we've identified in our research.
22:46
There are four opportunities on the slide you see here for MA plans to make an impact.
22:54
Each focus on different aspects of the transition process #1 targeting the handoff, not the readmission.
23:02
Focusing upstream is clearly a better way to identify root causes #2 improve transition communication with provider partners so we can align on what must be shared, how, and that when.
23:17
3.
23:17
Align transition support with trusted messengers.
23:21
Guidance from plans may be most effective when it comes through trusted providers.
23:27
And four, prioritize high risk members and moments targeting resources where they're most needed can drive the most impact.
23:36
We'll go through each one of these four points in more detail, talking about the specific problem, some options, and the potential benefits.
23:44
And I want to be clear, this is not prescriptive guidance, but rather just some ideas that you can consider.
23:51
Our hope is you'll walk away from this conversation with a few things you want to discuss with your team and see how they might benefit you.
24:04
So first let's consider how to target the handoff, not the readmission.
24:09
So what are we solving for here?
24:11
Most MA investment and care transition remains downstream, meaning it happens after the members already returned home or entered post acute care.
24:20
By this point, most of the high impact decisions have already been made and often without sufficient clinical or contextual insight.
24:30
The most consequential failures occur at the handoff because this is when accountability for the patient shifts either from the hospital team to the pack provider or from the provider team to the members caregiver.
24:44
Structural barriers like delayed discharge planning or pre authorization also increase this risk.
24:50
Here are some options to resolve this.
24:53
First, consider streamlining the pre authorization process by making sure requirements are clearly communicated to acute and post acute facilities.
25:05
Make determinations quickly.
25:07
Why?
25:07
Because it helps ensure the transitions the post acute care happen in a timely manner for everyone involved.
25:14
Second, share information with members and families.
25:18
They can make better decisions and quicker decisions when they have clear, accessible information about provider quality and network options.
25:26
The big benefit of focusing upstream is that it helps you identify root causes earlier in the process, not just respond to outcomes.
25:34
And that gives time to adjust to avoid any unnecessary readmission.
25:41
So you might identify there's an incomplete information transfer, unrealistic care plans, or misaligned recovery expectations.
25:49
If this isn't identified into a member has to be rehospitalized, then you don't have the opportunity to address it.
25:56
Additionally, planning early, especially for members with elevated clinic or social risk like a decent members, can reduce time pressure on care teams to evaluate posted care options, caregiver capacity and service need.
26:12
Our next opportunity builds on that, focusing now on communications.
26:26
One big challenge that emerged as the research team was looking at this topic is consistency in communication.
26:33
There isn't always alignment on what information needs to be shared or when.
26:38
Unclear and uncommunicated discharge plans, some medication changes, pending test red flags, or even follow up needs in the first few days after discharge can create avoidable gaps.
26:51
And those gaps lead to poor clinical outcomes and higher medical costs.
26:56
And the challenge is magnified when organizations use different or unconnected Ehrs, which is often the case between acute care and pack facilities.
27:07
Health plans and providers do not have an agreed upon standardized approach to what information must be shared, when it must be delivered, and how it will be packaged.
27:17
The opportunity here is to establish more consistent standardized processes, including shared expectations.
27:24
For example, creating a shared discharge summary template so that the receiving teams reliably get the same content in a consistent format.
27:34
It should include key details such as medication changes and reconciliation status, pending tests, risk flags, and required follow up.
27:44
Make sure everyone use shared metrics for early post discharge outcomes and stratification for discharge complexity and social risk.
27:53
For example, metrics like 7 day Ed visits, 7 to 14 day readmissions, or even tracking the medication discrepancies resolved and follow up visits completed can all be useful as early indicators of care transition challenges.
28:09
Additionally, building formal feedback process to identify when care transitions fail so gaps can be addressed prospectively rather than flagged only after utilization occurs.
28:23
Finally, enabling reliable information exchange across settings and information technology.
28:29
For example, naming a point of contact at each receiving site.
28:33
Considering filling prescriptions before the member leaves the facility in conducting follow up outreach after the member is home to confirm that home health has started, DME has arrived, and that the primary care visits have been scheduled.
28:48
Also, identifying coordination supports like transportation, meal resources, and community resource referrals are important so when communication is more reliable, care teams can act earlier with greater confidence.
29:02
Establishing a shared set of expectations that it should ensures that care teams receive timely and accurate information to make informed decisions.
29:13
While this opportunity is about communication with provider partners, the third opportunity focuses on how guidance reaches members.
29:28
So even when plans provide strong support, it may not be effective if it is entrusted.
29:34
Sometimes MA plans find that their impact may be limited by the lack of trust from member and caregivers at discharge.
29:42
During stressful transitions, members and caregivers often prioritize guidance from clinicians they know over outreach from a health plan they don't see as intimately involved.
29:53
I can tell you as a clinician, I've experienced that a lot personally where patients, family members will say I know the doctor told me this or this person told me, but you know me best, you've been working closely with me.
30:05
What do you think?
30:07
There really is trust in the people that are closest to these members during their experience in post acute care.
30:14
And receiving outreach from multiple messages can confuse the members and the caregivers, especially if the guidance doesn't always align.
30:23
So to address this, consider how to align with those trusted messengers.
30:27
Now, this opportunity is going to look different depending on your specifics and the relationships you have with your provider partners.
30:34
But some ideas could be supporting hospitals and implementing discharge risk screening benefits or navigation support routed through case management.
30:44
And then finally, a dedicated transition coordinator aligned to the unit.
30:49
There has been some research that has shown that care teams dedicated to transitions can improve care transition outcomes and lower readmissions.
30:58
I'll share a quick personal example.
31:00
My mother-in-law was recently spent a few days in a Pittsburgh hospital for treatment of AGI problem.
31:06
At the time of discharge, she was provided with written discharge instructions by the bedside nurse, but it was a dedicated discharge nurse who thoroughly reviewed the discharge instructions with her by video and then patiently answered her questions.
31:21
Despite the remote status of this discharge nurse, she was very knowledgeable about community resources and both my mother-in-law and wife felt well cared for and well prepared for what would happen after discharge.
31:35
Hearing about this experience really made me start thinking about how something like this may work in the Smith setting.
31:42
You can also think about how to Co design transition programs with provider partners so members experience a single coherent guidance pathway.
31:52
And finally, consider how to provide plan insights to trusted clinicians and staff who council members.
31:58
This helps clinicians make more informed recommendations and doesn't increase the decision making burden for the member.
32:06
The goal is to create a more unified experience for the member.
32:10
We want to see increased uptake of plan and provider guidance and that can happen if the information comes from a primary trusted resource.
32:19
Aligned communication can also help reduce confusion and the burden that members and caregivers experience when they attempt to navigate care transitions.
32:30
So the final opportunity we'll talk through is about drinking resources effectively.
32:45
Last big slide here.
32:47
And this opportunity starts with the agreeing that all, not all, care transitions carry equal risk.
33:08
Members of complex medical needs, of health conditions here, for social barriers, they're all discoursed fears when the location issues.
33:39
This means that you one-size-fits-all care transitions, different risk, and all resources.
33:52
This isn't unique to transition of care of course.
33:56
Many of you are likely focused on population health and diet based care efforts, which also consider how to stratify risk and ensure that you get the right resources and the right to the right members.
34:07
We can also apply that same technique or logic here, again, without being prescriptive.
34:13
There's some possibilities for you to consider conducting high touch interventions in the highest risk window when rapid course correction is still possible, matching the intensity of support to the setting so it's proportional.
34:30
So for example, a sniff in a home health setting may require very different levels of outreach.
34:37
And lastly, target resources where they're most likely to prevent complications, improve the member experience, and really stabilize quality performance.
34:48
All this allows for more effective interventions and avoid spreading resources too thin.
34:54
It's really a more thoughtful approach that reflects that each member is different.
35:01
That wraps up our last opportunity, and I'll turn it back to Miriam to bring our content to a close before we take your questions.
35:13
Great.
35:14
Thank you, Jeff.
35:15
Again, hope you have been thinking through your questions.
35:20
As Jeff and I have been speaking, we encourage you to pop them into the questions panel so that we can get to as many of them as we can.
35:28
But before we do that, I want to just take a moment, recap what we've covered today, as well as remind y'all of the key insights that we hope you walk away with.
35:38
So as a reminder, we started by looking at the why.
35:41
We looked at why transitions of care are challenging for all stakeholders involved and really thinking about what the consequences are when those handoffs just don't go as planned.
35:56
Then we looked at the process for patients moving from that acute care to a post acute care facility, looking at each step of the way to see where those gaps were emerging with that specific lens of thinking about kind of where is that information gap contributing to some of these challenges.
36:19
And then just a few moments ago, Jeff walked through some of these opportunities for you all to consider to improve transitions of care.
36:28
Thinking about kind of a range of opportunities from, you know, where how to think about the handoff, not just the readmission, how to think about transition communication, how to really think it, how to think about aligning support with those trusted messengers, and finally, really how to prioritize resources best.
36:55
And so couple of things that I really hope that you take away from today.
37:00
First, I hope you think about that by focusing on the handoff as a whole instead of just readmissions as a single metric, MA leaders can really shift transition management from reactive to proactive and ultimately be a more reliable moment in the care journey.
37:19
Ultimately, this improves the quality of sight of care decisions, reduces preventable complications, and just overall makes the member experience more cohesive and better for them, and hopefully helps them get back to their home as soon as possible.
37:36
Second, there are real opportunities to strengthen these transitions of care moments and ensure that the next care setting receives timely clinical and contextual insight.
37:48
This is not an insurmountable problem, and narrowing that accountability gap as patients transition is really a worthwhile thing to consider.
38:00
Finally, it's really critical to focus on opportunities to reduce inappropriate readmissions and ensure appropriate care.
38:11
But again, it encourage you all to remember that readmissions are often a lagging indicator and may hide the root cause and solving for those root causes is ultimately how the industry improves transitions of care.
38:27
So with that, let's take your questions.
38:28
I know we have a few that have been submitted already, but encourage you all to submit some more as we are answering.
38:38
So one more slide.
38:44
All right, Jeff, I can read the first one if you want.
38:50
Sure.
38:51
All right.
38:51
So the question is how do we measure success if we're shifting away from readmissions as that primary metric?
39:04
Steph, do you want to tackle that one?
39:07
Sure.
39:08
So what I would say is readmissions don't matter, but we really have to think about, you know, focusing upstream.
39:15
They're lagging indicators.
39:19
Indicators again, it's it's too late to really make an impact.
39:23
So things to focus on again are the, the timeliness and the completeness of the handoff.
39:29
You know, early as we've discussed and resolving any of the care we've discussed include medicines and even things like transportation and food that I personally find are very important because when they discharge home from post acute care and are really often overlooked.
39:48
And then again, looking shorter term, instead of focusing on readmissions, let's look at, you know, what happens in the 1st 7 to 14 days home.
39:57
Do the members have the resources they need?
39:59
Do they have the, the, the home health service, the DME equipment, the follow up on physician visits?
40:06
And again, over time, if we focus on those upstream things, we will see that readmissions will be reduced and the member experience will be improved as well.
40:20
Next question that we have is a real kind of practical on where should plans start if they want to have the kind of biggest impact quickly.
40:32
I'm happy to to tackle that one.
40:35
I think we've talked about this a bit, but really encouraged to start at the handoff, start at that moment of transition of care and not downstream.
40:46
And so focus on one high friction point.
40:50
Is it discharge?
40:52
Is it the moment of, you know, going from the sniff to home health?
40:57
Is it something else?
40:59
But really think about kind of 1 moment.
41:02
And then within that moment, what are two to three things that are operational that you can change?
41:07
Is it thinking about the pre authorization process and how to create a faster clearer process?
41:14
Maybe it's consistent hand off expectations with partners.
41:20
Maybe it's you know, who's the right contact across settings.
41:23
I think there's a number of different levers that you can pull, but focus on a couple to start and then pilot it like like many programs, really thinking about kind of a small set of provider partners first rather than kind of rolling it out system wide to see what might work and and what might not.
41:42
And then finally, you have to measure it, right?
41:43
We have to see if it works.
41:45
So think about, you know, what are some process metrics?
41:48
Is there timeliness, completeness, because you know, those outcome changes are going to take a little bit longer.
41:56
So really thinking about those process metrics, monitoring them, seeing what needs to be changed before expanding to kind of more opportunities or more places throughout the system.
42:09
Anything you'd add, Jeff?
42:11
Nope, I think you got it.
42:13
Great.
42:14
Let's see one.
42:15
Here's another one.
42:17
Curious if we can highlight a successful Co design of a transition of care around specific diagnosis with an identified sniff provider.
42:28
Jeff, I'm wondering if in your experience you have anything that might fit there?
42:34
So another questions about sniff providers, I can tell you the first thing that comes to mind is home health providers during that transition that, you know, patients with a diagnosis like CHF that really, you know, have some risk when they transition home if they don't have the right support.
42:51
Where that Smith provider they they work with home health providers that have clinicians that that have experience and have care plans that are really focused on educating those CHF members on their disease process and even being very proactive in making sure they have follow up with their PCPS and any specialist after that.
43:12
So that that's what comes to mind.
43:15
I've seen that in in a certain market where again, that pack provider has a trusted partner in the home health agency that can not only get in there and have the, excuse me, the start of care completed timely, but then also can share the educational materials.
43:33
And it just the the proactive approach of the clinicians and the agency to make sure the members needs are met and there's no gaps that would result in that member back in the EDM potentially readmitting.
43:46
Yeah, that's a great example.
43:51
All right, we have a few more questions so folks still have a chance.
43:54
If you have some other ones that you've been thinking about, please do submit them so we can again get to as many as we have time for.
44:01
Another question that we have here is, you know, if readmissions are a lagging indicator, as I think I've said at least three or four times, you know, why have they been such a, a focus historically?
44:16
I'm happy to to tackle that one.
44:18
I think that readmissions have been a focus because you know, they're measurable, they're comparable across organizations and and of course they've been kind of directly high to cost and quality metrics.
44:33
And so because of that, you know, they provide a clear signal moment of failure and that makes them a really logical starting point.
44:44
And again, I think we've said this again many times, but you know, the the point is not to stop measuring readmissions.
44:50
I think it's incredibly important to continue to do that.
44:53
But the challenge is they don't really indicate where something broke down.
44:57
They only indicate the ultimate kind of failure at point at the at the end.
45:02
And so, you know, for plans and provider organizations who are invested in really managing the outcome, it doesn't really fix that kind of underlying process.
45:16
And so the shift now, and I think what we've been, you know, commenting on today is kind of how do you keep readmission as that metric, but really pair it with some other process improvements, with some other metrics.
45:31
So not stop measuring, but really add to it.
45:33
And I think we've given a couple examples of, you know, some of the other metrics that you can measure along with readmissions to really think about kind of the process more holistically.
45:48
All right.
45:48
I think the moment we've got one more, so we'll answer that one.
45:52
And again, folks can can put in a couple more questions if you've got them.
45:57
So last question that we've got right now is, is the information gap, you know, that we've been talking about today really new or you know, has it always been there?
46:08
Jeff, I don't know if you want to comment on this one based on kind of your experience in the field.
46:13
Sure.
46:13
So again, I think we're all aware it's, it's not new, it's been there for a long time.
46:19
The big thing that has changed is, is the impact and really the visibility we have into the gaps.
46:26
Part of that is due to just because of the complex nature of the patient populations that we've discussed earlier.
46:32
And another thing we discussed earlier is the greater post acute care utilization.
46:37
So those those two factors just make it much more visible.
46:40
There's also higher expectations for care coordination and outcomes, a lot of pressure to have smooth handoffs and and drive positive outcomes.
46:49
And as as we've talked it, it's more fragmented.
46:53
There seems to be more handoffs for an individual member as they move through the process.
46:59
At the same time, there's more pressure on cost and performance.
47:03
So the gap feels really more urgent, especially to where MA plans, not because it's new, but because the consequences are larger and they're really harder for the health plans to absorb.
47:16
Yeah, I think that's great.
47:17
I think you know the the what Jeff presented earlier about the kind of growth of the MA population and the growth of post acute care utilization, I think really speaks to that rate that this isn't new, but it's it's certainly getting rising in prominence and importance.
47:34
I think that that is all the questions we have.
47:40
So appreciate everyone's time today and appreciate you all joining.
47:45
Have a really great rest of your day and thank you so much.
47:48
Thank you, Thank you to our speakers, and thank you for that great presentation and for sharing your thoughts.
47:59
Thank you to the audience for participating in today's webinar.
48:03
This concludes today's presentation.
48:06
Thank you again and enjoy the rest of your day.
Why post-acute transitions remain high risk
Care transitions from acute to post-acute settings are some of the most complex moments in the member journey. As patients move between settings, accountability shifts to a new team at the same time clinical and social risk often rise. When information is incomplete, backward-looking or poorly contextualized, providers may be forced to make time-sensitive decisions without the full picture they need.
Historically, organizations have focused on reducing hospital readmissions. The webinar reframed that metric as an important outcome — but not the whole story. The bigger issue is often the clinical handoff itself: what information travels with the member, what context is missing and where coordination breaks down before complications appear.
See how our post-acute care solutions can help
Related healthcare insights
White paper
Incomplete, backward-looking information during care transitions drives avoidable utilization. Learn why MA plans must focus on the handoff, not just readmissions.
Video
Supporting care, reducing stress, and serving as a point-of-contact are just a few of the benefits care coordinators offer.
Case study
See how a leading health plan reduced costs, improved outcomes and strengthened provider relationships with a modern post-acute care model.