Polypharmacy: A large and growing problem in the workforce
38 million working Americans are at-risk for complications due to overprescribed medications.
Polypharmacy can mean simply that one person is taking multiple medications at the same time. In some cases, there may be sound clinical reasons for taking each of those medications.1
However, polypharmacy usually refers to times when these additional medications may be unnecessary or even harmful.2 The concern is that a lack of oversight can lead to a harmful form of polypharmacy, where overprescribed or misused treatments could bring about negative health outcomes.
What exactly constitutes polypharmacy can vary. For example, studies show that patients who take more than four medications have an increased risk of injury from falls, and that risk rises with each additional medication.3 In this paper, Optum Rx defines polypharmacy as when one person uses five or more chronic prescription medications.
Polypharmacy has negative consequences for patients and the healthcare system. These effects can include increased risk for adverse drug events, increased hospital readmissions and even increased mortality.4 The independent Lown Institute predicts that inappropriate polypharmacy will cost the system an additional $62 billion over the 2020–2030 period.5
Polypharmacy has been widely studied and reported, even in mainstream media outlets like the New York Times.6 But the vast majority of this attention is focused on older patients (age 65+).7
However, the potential problems related to polypharmacy can affect people of any age. For example, its presence among the younger, working-age population is less well publicized but is significant. While more than half of adults 65 and older take four or more prescription drugs, 24% of all adults under age 65 do, as well.8
Roughly 157 million of the total U.S. working age population (~201 million) are currently in the paid workforce.9, 10 Applying the 24% polypharmacy rate for this age group, that means nearly 38 million workers may be at-risk for the harm associated with polypharmacy.
38 million people in the active U.S. workforce of 157 million are at-risk of polypharmacy (24%).
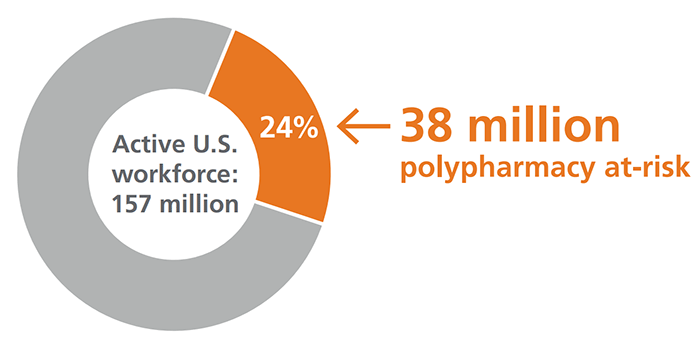
Image citations: 24%: Kaiser Family Foundation. KFF Health Tracking Poll Prescription Drugs. Published March 1, 2019. 157 million: U.S. Census Bureau. Aging Boomers Solve a Labor Market Puzzle. Published June 21, 2021.
And the problem is getting worse. One recent paper showed that the incidence of polypharmacy more than doubled during the five-year period it studied, and this increase was not limited to the elderly.11
Working age adults have been described as “…the undoubted economic engine for the country.”12 Common sense tells us that the health and wellbeing of this critical age group impacts not only their personal quality of life but also the dynamism of every workplace and the health of the entire economy.
In summary, employers and plan sponsors can no longer afford to think about the potential harms of polypharmacy as strictly a problem for those who have aged-out of the workforce.
In this article we want to take a closer look at when polypharmacy has a negative impact. We’ll examine how it happens, how much it costs, and what, if anything, employers and plan sponsors can do about it.
We can begin by recognizing that the healthcare system is very well designed for starting medications, but not for reducing or stopping them.13 And, as noted, at least some patients may need five chronic drugs or more. For example, some of the biggest increases in utilization have occurred in preventive medications, such as cardiovascular drugs.14
Yet with each additional medication, patients face up to 10% increased risk for an adverse drug event.15
Unfortunately, as we age, we may experience a natural increase in the number of treatable conditions, which leads to more medications being prescribed. As a result, we commonly see patients moving slowly towards polypharmacy.16
Here is where the siloed or fragmented U.S. healthcare system can play a damaging role. As a patient’s conditions become more complex, they will tend to interact with different health providers, perhaps including multiple specialists. This creates a growing number of individuals who may prescribe medications.
When patients receive prescriptions from multiple prescribers who cannot access the patient's complete medication regimen, we see a rising risk for adverse drug events. For example, we may see drugs prescribed that should not be used with other drugs or using one drug to treat the side effects of another drug, duplicate therapies, or even unnecessary treatments.
Polypharmacy has significant costs, both physical and financial.
In clinical terms, polypharmacy:
- Contributes to increased adverse drug events and drug-drug interactions, as well as decreased medication adherence17
- Is associated with adverse patient outcomes and even hospitalizations18
- Has a statistical relationship with mortality19
- Can lead to adverse drug events accounting for more sickness and death than most chronic diseases, with death rates even higher than many common cancers20
- Is associated with an incremental increased risk for thirty-day hospital readmission per each additional drug prescribed.21
These cumulative clinical impacts are expected to result in at least 4.6 million hospitalizations and nearly 150,000 premature deaths in the U.S. between 2020 and 2030.22
In financial terms, polypharmacy is a major contributor to total adverse drug event-related costs, new medical conditions caused by overprescribing, or both. These events accounted for $528 billion in 2016 — equivalent to 16% of total U.S. healthcare expenditure in that year.23
Costs associated just with inappropriate polypharmacy are projected at approximately $62 billion over the 2020–2030 period.24
And yet the most important thing to remember is that this is the very population that employers — and society — rely on the most: working people in their prime. We need them not just to show up, but to deliver energy, creativity and initiative.
However, that kind of high performance could be inhibited by effects associated with harmful levels of polypharmacy, like increased adverse drug events and millions of additional hospital stays and outpatient visits.
Therefore, let us turn to some practical steps to mitigate polypharmacy, or better yet, prevent it from happening.
It makes sense to target the working population for polypharmacy, as the road to potentially harmful medication overload begins sooner than you might suspect. Polypharmacy is mainly concerned with chronic medications, and many chronic conditions begin relatively early in life. For example, the average first onset for type 2 diabetes is age 45, while almost half of adults over the age of 20 have elevated or high blood pressure.25, 26
One advantage of addressing this age group is that younger adults are more likely to already be actively involved in managing their medications, compared to older adults. This means they tend to be open to any potential interventions.27
But what would we need for an effective polypharmacy intervention program? For one thing, do we even know how to treat polypharmacy? And if so, how can we cope with the huge number of working age individuals who may — or may not — need intervention?
The answer to the first question is a resounding “yes.” Thanks to the intense focus on polypharmacy among the older population, there is already a robust array of proven techniques to help people untangle their medication burden.28 Furthermore, these techniques can be adapted to suit the somewhat different needs of working age people.29
The main approach can be very simply described as the process of adjusting medications down to the minimum effective dosage. Or it may involve stopping a given prescription when a patient's health status changes in a way that the potential for harm from a drug or drugs does not outweighs their benefit.30
This approach — sometimes called deprescribing — is not intended to be in any way a coercive, top-down technique. Rather, it requires shared decision-making that involves the patient, pharmacist, and doctor in a collaborative effort to deliver the best quality healthcare.
For example, recall what we said earlier about how the fragmented care system prevents providers from having an accurate picture of a patient’s total healthcare. This process begins with a detailed medication review, in which a pharmacist specifically evaluates a patient for polypharmacy.
In other words, the first step is to re-integrate the patient’s care profile. Only then can the broader care team begin to look for opportunities to stop, adjust or change medications that are potentially harmful or that no longer benefit the patient.
But for all the undoubted benefits of a detailed medication review, conducting 38 million of them simply isn’t practical (or necessary). A far more targeted approach is required, one that applies integrated pharmacy and medical data to identify members most likely to benefit from a prescription checkup.
For example, this kind of data can identify individuals using five or more chronic medications, with three or more from categories known to include deprescribing opportunities.
What employers need, then, is a comprehensive program that can help their plan members get to the correct number of medications, at the appropriate dose, for the right amount of time.
Every employer or plan sponsor should carefully consider the new Optum Rx® Polypharmacy Value Management Program. This program uses the extensive Optum Rx case management infrastructure to engage members taking five or more chronic medications — including three or more within 20 targeted, clinically supported drug classes.
Eligible members receive a comprehensive medication review to see if there are any medications that present a lack of efficacy, side effects, or known interactions. As part of the review, we also ask the member if they see any value in continuing to use a particular medication.
With this information in hand, we can then rely on proven collaborative techniques. These include sharing decisions among the pharmacist, member, and provider, and then engaging the provider to evaluate and take any appropriate action.
Finally, because the polypharmacy program is embedded within our overall case management, the system can automatically monitor ongoing medication use and detect any changes. This helps keep all the stakeholders fully informed and alert to any recurring or new problems.
Early results show that the program will not just meet but exceed our expectations. Early proof of concept results showed strong member participation. In the 6-month pilot period, we had 12.5% of members engage with a pharmacist. Based on the pilot results, we project a 25% member engagement rate for a full-year program.
Also, the pilot results showed providers were accepting recommendations and stopping, switching, or adjusting medications 40% of the time, based on the data we provided. The result is an average total cost savings of more than $1,300 per successful intervention.31
Optum Rx customers are increasing their emphasis on the importance of complex member management and high-cost member management. The Optum Rx Polypharmacy Value Management Program meets both those needs. By leveraging the huge data capabilities of Optum to efficiently identify opportunities to address medication overload, our clients can take a more proactive approach to address polypharmacy at a younger age.
Ultimately, our goal is to help members take more ownership of their own health, lower the risks and costs associated with clinically unnecessary or unwarranted treatment, and potentially lower their medication costs.
To learn more about how the Optum Rx Polypharmacy Value Management Program can benefit your organization, please contact your consultant or Optum Rx representative.
Related resources
Article
Straight-through processing connects virtual card payment and remittance data to reduce manual reconciliation and keep receivables moving.
Case study
See how a health system reduced excess inpatient days and improved flow with earlier intervention and aligned care teams.
Article
John Hoffman, VP of Product at Optum, discusses how the future of payment integrity is built on preventing errors before payments are made.
- BMJ Open Quality. Deprescribing for all: a narrative review identifying inappropriate polypharmacy for all ages in hospital settings. First published July 6, 2021. Accessed September 15, 2021.
- ibid.
- American Family Physician. Polypharmacy: Evaluating Risks and Deprescribing. Published July 1, 2019. Accessed October 1, 2021.
- BMJ Open Quality. Deprescribing for all: a narrative review identifying inappropriate polypharmacy for all ages in hospital settings. First published July 6, 2021. Accessed September 15, 2021.
- Lown Institute. Medication overload: America’s other drug problem. April 2019. Accessed September 16, 2021.
- New York Times. Looking to Tackle Prescription Overload. Published June 7, 2021. Accessed September 15, 2021.
- PLOS One. Trends in polypharmacy and dispensed drugs among adults in the Netherlands as compared to the United States. Published March 22, 2019. Accessed September 15, 2021.
- Kaiser Family Foundation. KFF Health Tracking Poll Prescription Drugs. Published March 1, 2019. Accessed September 15, 2021.
- National KIDS COUNT. Adult population by age group in the United States. Population Estimates, U.S. Census Bureau. Updated September 2020. Accessed September 15, 2021.
- U.S. Census Bureau. Aging Boomers Solve a Labor Market Puzzle. Published June 21, 2021. Accessed September 16, 2021.
- PLOS One. Trends in polypharmacy and dispensed drugs among adults in the Netherlands as compared to the United States. Published March 22, 2019. Accessed September 15, 2021.
- Ukhanova, Maria. Care Coordination and Polypharmacy among Working-Age Adults with Multiple Chronic Conditions. (2017). Texas Medical Center Dissertations (via ProQuest). Accessed September 15, 2021.
- American Family Physician. Deprescribing Is an Essential Part of Good Prescribing. Published January 1, 2019. Accessed September 16, 2021.
- PLOS One. Trends in polypharmacy and dispensed drugs among adults in the Netherlands as compared to the United States. Published March 22, 2019. Accessed September 15, 2021.
- Lown Institute. Medication overload: America’s other drug problem. April 2019. Accessed September 16, 2021.
- BMJ Open Quality. Deprescribing for all: a narrative review identifying inappropriate polypharmacy for all ages in hospital settings. First published July 6, 2021. Accessed September 15, 2021.
- ibid.
- ibid.
- ibid.
- ibid
- BMJ Open. Risk of 30-day hospital readmission associated with medical conditions and drug regimens of polymedicated, older inpatients discharged home: a registry-based cohort study. Published July 14, 2021. Accessed September 16, 2021.
- Lown Institute. Medication overload: America’s other drug problem. April 2019. Accessed September 16, 2021.
- Annals of Pharmacotherapy. Cost of Prescription Drug-Related Morbidity and Mortality. Published Sept. 1, 2018. Accessed September 16, 2021.
- Lown Institute. Medication overload: America’s other drug problem. April 2019. Accessed September 16, 2021.
- Healthline. Age of Onset for Type 2 Diabetes: Know Your Risk. Last updated on July 6, 2018. Accessed September 17, 2021.
- Houston Methodist On Health. Why Your Blood Pressure Matters — Even in Your 20s & 30s. Published January 22, 2020. Accessed September 17, 2021.
- BMJ Open Quality. Deprescribing for all: a narrative review identifying inappropriate polypharmacy for all ages in hospital settings. First published July 6, 2021. Accessed September 15, 2021.
- US Deprescribing Research Network. What We Do. Accessed September 17, 2021.
- BMJ Open Quality. Deprescribing for all: a narrative review identifying inappropriate polypharmacy for all ages in hospital settings. First published July 6, 2021. Accessed September 15, 2021.
- American Family Physician. Deprescribing Is an Essential Part of Good Prescribing. Published January 1, 2019. Accessed September 16, 2021.
- Optum Rx internal data: January – June 2021. Results are illustrative and are not guaranteed.