Explore insights by category
Data and analytics | Finances and payments | Mental health | Patient and member engagement | Pharmacy care | Pharmacy management | Technology and automation | Value-based care | View all
Latest featured insights

Article
Learn how health plans can fill care gaps by offering greater support and personalized solutions for women experiencing menopause.
![A Quarter-Century of Pharmacy Benefit Changes [E-Book]](/content/dam/optum-dam/images/business/pharmacy/hand-with-vial-1080x720.jpg)
E-book
Explore the dramatic changes in the years since 2000 — in drug performance and design, and especially affordability.

Article
Explore how evidence-based tools like The ASAM Criteria® Navigator and InterQual® Substance Use Disorders Criteria are helping payers and providers efficiently and effectively navigate the complex substance use disorder landscape today.
![Automation Strategies for Empowering Staff and Patients [Webinar]](/content/dam/o4-dam/images/professionals/company-meeting-1080x720.jpg)
On-demand webinar
Learn how to help transform hospital revenue cycle operations with healthcare automation.
Data and analytics

Article
Understand how routine clinical practice impacts information captured in real-world data (RWD).

On-demand webinar
Hear from experts in this Endpoints News webinar on the increasing importance of clinicogenomic data, including diverse phenotypic and genotypic profiles.

Video
Optum Life Sciences leaders break down common missteps when using RWD and how to create practical strategies to overcome them. Watch the video from STAT Summit.

Article
Providers collect data about patients every day. But what should they be considering — and doing — to put their clinical data to good use?
Finances and payments

Article
Discover 4 ways health plans can save money today — and in the future — by engaging with a digital claim payment partner.

Article
Learn how AI is changing the fraud case review process.
Article
The connection between money and health runs deeper than just costs — your employees rely on your benefits strategy for overall wellness.
Article
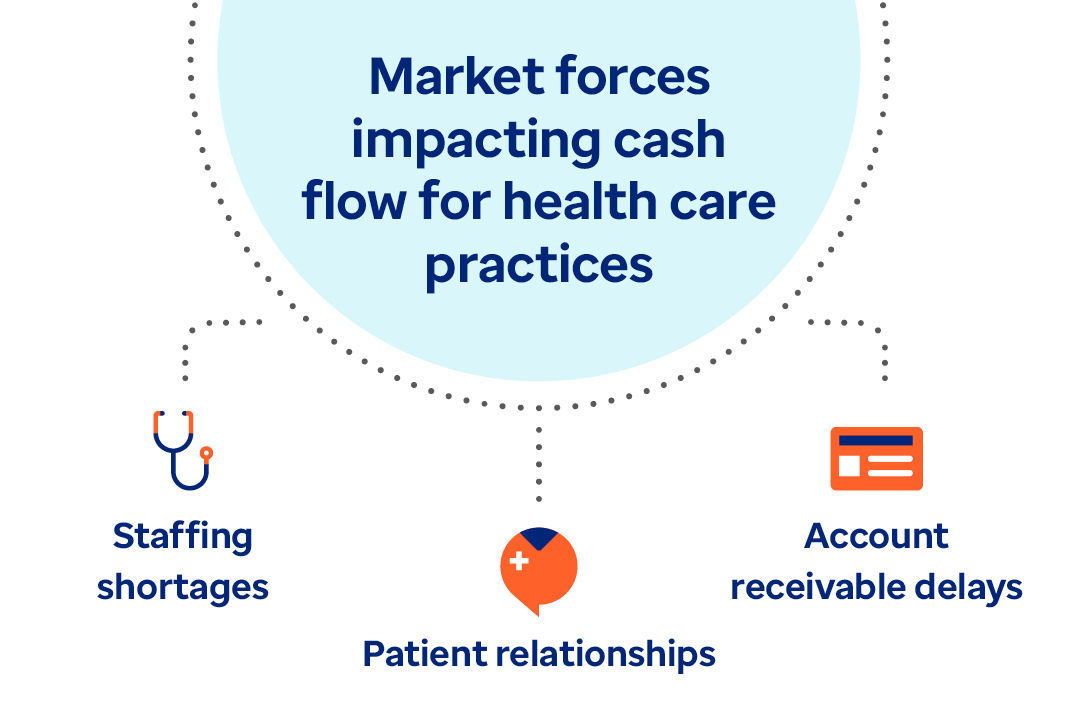
Learn how payment delivery optimization can improve the healthcare financial cycle and bridge the gap between payers and providers.
Mental health
![Behavioral Health Support Helps Improve ROI [Case Study]](/content/dam/optum-dam/images/business/insights/therapist-conversation-1080x720.jpg)
Case study
With work-life balance becoming a priority, offering no-cost outpatient therapy is more than a benefit — it’s a commitment to wellbeing.
![Reimagining behavioral health: Smarter solutions [Webinar]](/content/dam/optum-dam/illustrations/desk-with-laptop-1080x720.png)
On-demand webinar
Join speakers Lou Dierking and Miranda Anderson as they share insights into how technology can drive much-needed improvements in behavioral health care.
![Leveraging GLP-1s Within a Whole-Person Approach [Webinar]](/content/dam/optum-dam/images/business/insights/plus-size-woman-smiling-1080x720.jpg)
On-demand webinar
A holistic, strategic approach to GLP-1s combines medication, surgery and behavioral health to support weight management and reduce costs.
![Support for Substance Use Disorders [White Paper]](/content/dam/optum4/images/ohb-sud-wp-adaptive-image-1080x720.jpg)
White paper
Expand access to evidence-based support to help individuals achieve stabilization and sustain recovery.
Patient and member engagement

Article
Learn how Optum Serve is helping to advance the health and well-being of Veterans and spouses in the trucking and cybersecurity workforce.

Guide
Learn how Optum Serve helped Veterans achieve health and wellness goals, promoted well-being, prevented illness and reduced the burden of chronic conditions.
White paper
Learn how Optum Serve supports Veterans through a whole-health approach to work and life.

Case study
See how a leading health plan reduced costs, improved outcomes and strengthened provider relationships with a modern post-acute care model.
Pharmacy care

Article
How a specialty pharmacist ensures patient health and safety through education, screening for drug contraindications and check-ins with prescribing clinicians.

Article
When a breakdown in care left a patient without essential IV nutrition, learn how Optum Infusion Pharmacy stepped in with a new approach.

Stay up to date on our Specialty and Infusion Pharmacy offerings and get important industry developments delivered directly to your inbox.

Article
On average, Optum Infusion nurses spend approximately 1,300 hours per year providing care to patients. Hilary, an Optum Infusion nurse, knows this firsthand.
Pharmacy management

Article
Clear pricing. Aligned scale. Actionable insights — helping you make smarter decisions, faster.

Article
Discover the unique challenges and responsibilities of introducing AI into pharmacy benefit solutions.

Article
We delivered a seamless 1/1 transition for over 800 new clients with strong service, stable operations and improved member experiences.

Article
The move to Maximum Fair Prices for popular drugs will trigger new economic considerations for plan sponsors.
Technology and automations
Case study
Using digital integration to ease administrative burdens can help you spend more time with patients and deliver positive patient outcomes.

White paper
Read the white paper for strategies on controlling fixed costs, efficiency and organizational flexibility.

Case study
See how Lima Memorial improved efficiency with advanced technology.
On-demand webinar
Watch the webinar to learn actionable strategies on tackling decreased hospital margins, increased labor costs and staffing shortages.
Value-based care

Article
How employers and payers can step up with tailored benefits, workplace accommodations, and integrated care.

Article
There’s a lot at stake with organ transplant claims. Learn the importance of selecting an effective payment integrity approach.
Article
Learn how health plans can fill care gaps by offering greater support and personalized solutions for women experiencing menopause.

Article
A fresh approach to benefits is easing leaders’ administrative burden and connecting employees to better care.