Executive summary
Chimeric antigen receptor T-cell (CAR T) therapy is a transformative, gene-based immunotherapy for select blood cancers, offering curative potential for patients with relapsed or refractory disease.
Utilization trends
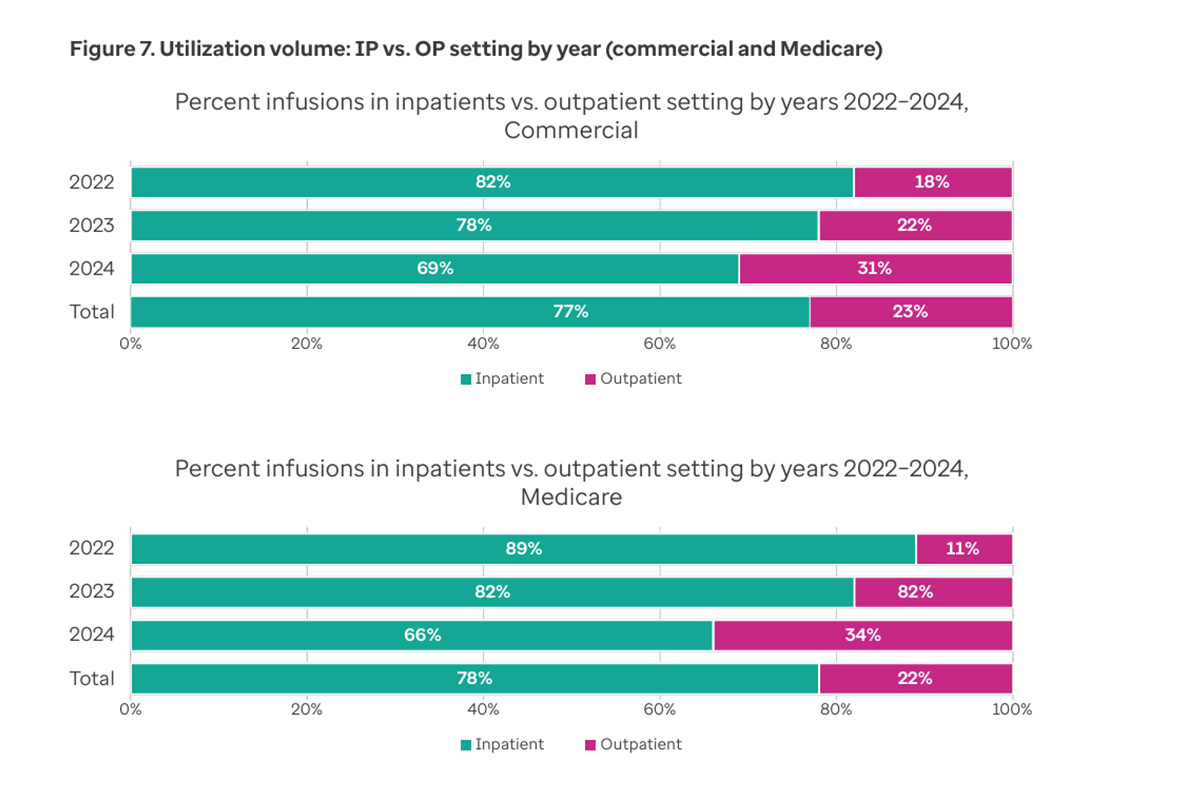
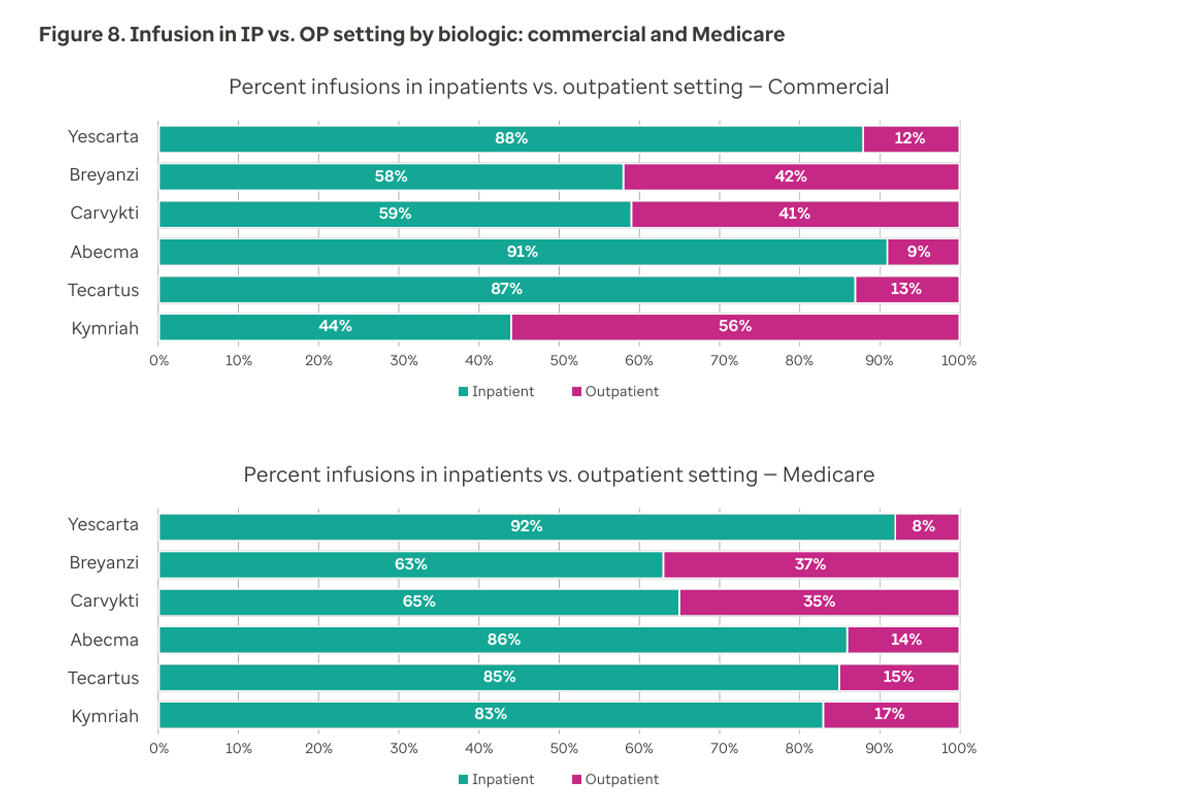
- A shift in CAR T therapy site of care from inpatient to outpatient can be observed in the utilization data. Based on our analysis of CAR T cases from 2022 to 2024, 31% of all the 2024 commercial cases are in the outpatient setting, compared with 18% in 2022.
- A similar shift toward outpatient setting (from 11% in 2022 to 34% in 2024) was also seen in the Medicare population.
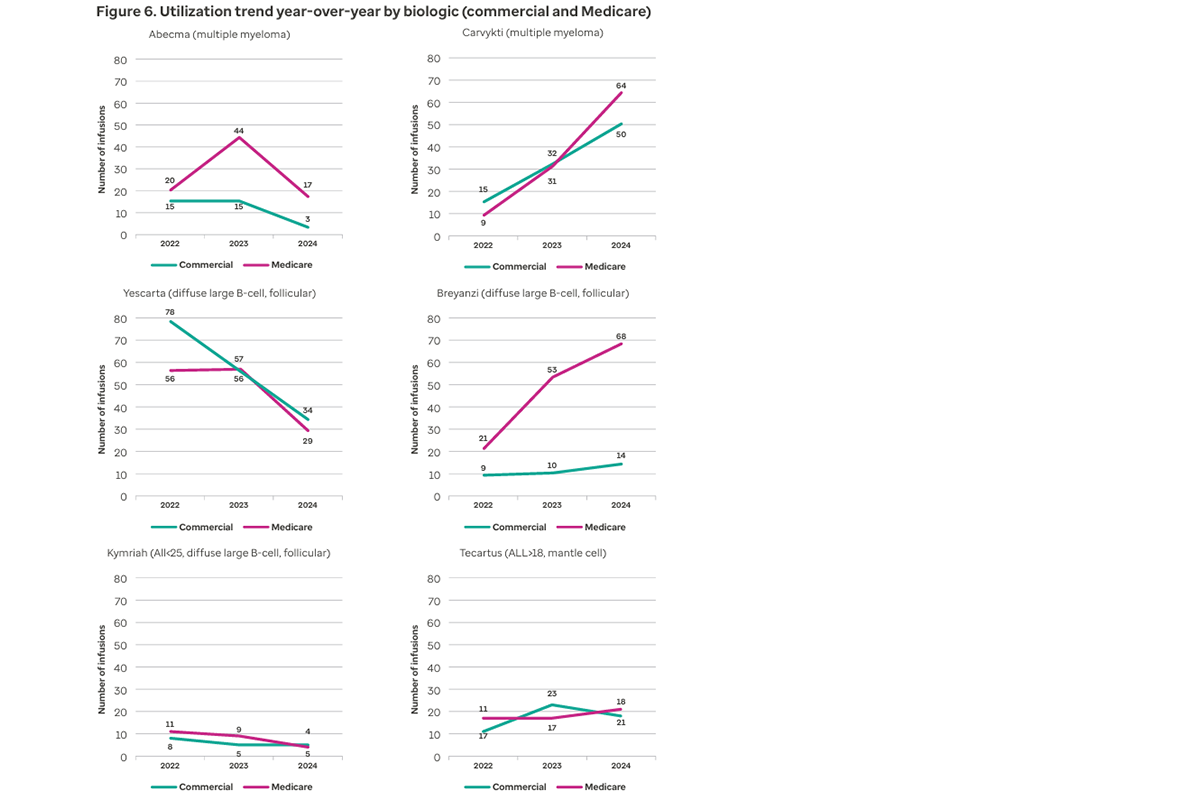
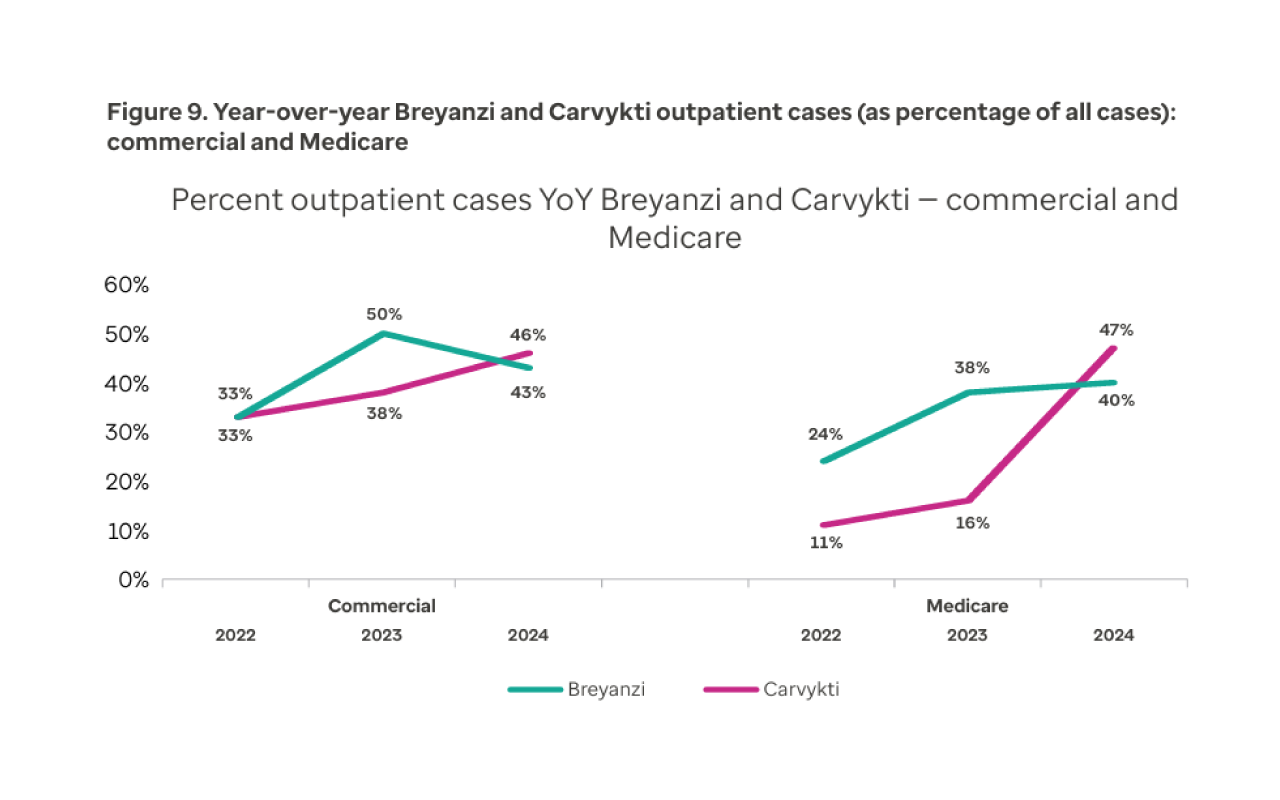
- Biologic utilization patterns continue to change as providers gain experience with certain biologics and new agents enter the market.
For diffuse large B-cell lymphoma, the use of Breyanzi® has increased over the analysis period, while Yescarta® has decreased for both the commercial and Medicare populations. For multiple myeloma, Carvykti® utilization has increased year-over-year, with decreased use of Abecma® in both the commercial and Medicare populations.
Post-infusion outcomes
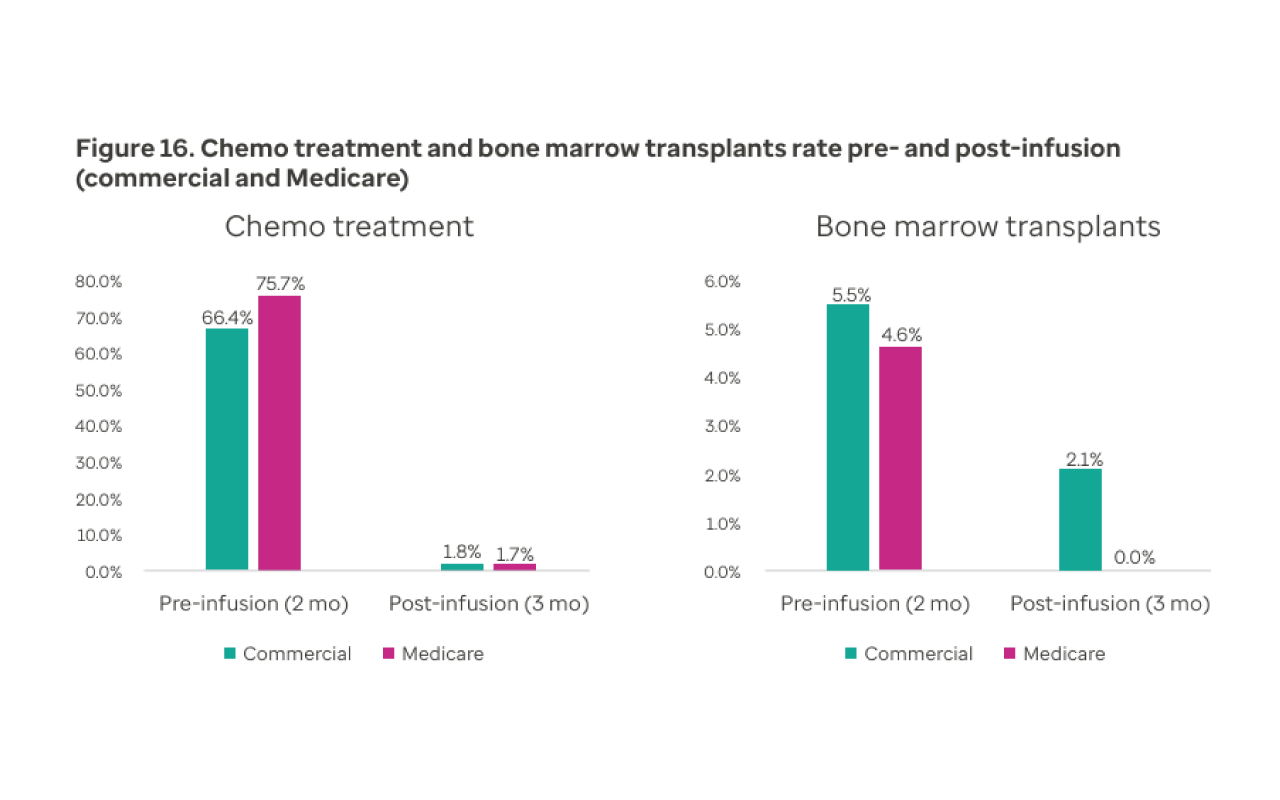
- Our data indicate CAR T therapy reduces the need for subsequent chemotherapy or bone marrow transplant. Only 1.8% of commercial and 1.7% of Medicare patients in our study needed chemotherapy within 3 months post-infusion. These findings support the efficacy of CAR T therapies in maintaining remission and are consistent with prior real-world analyses.1
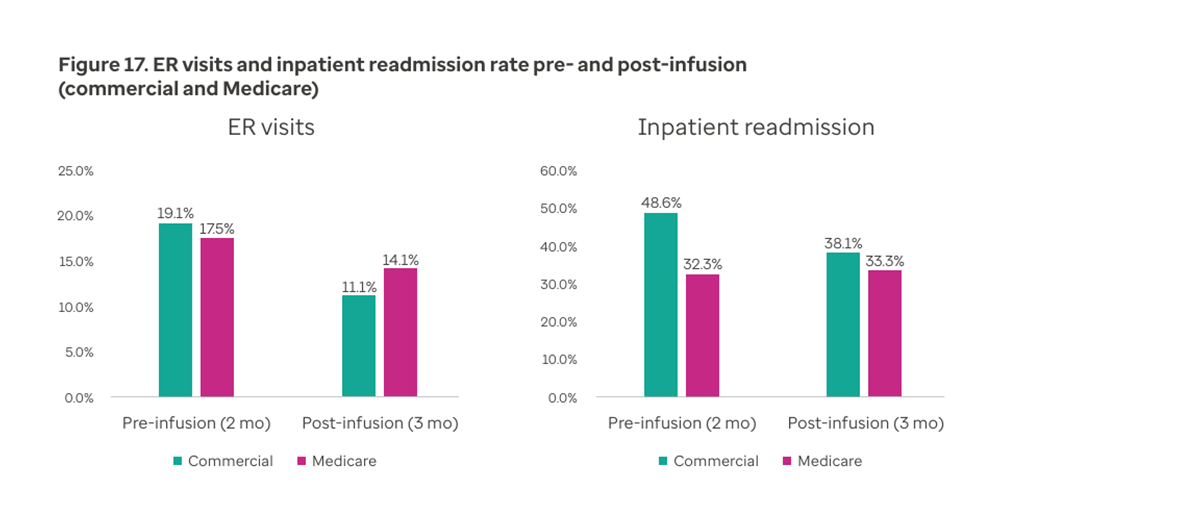
- Consistent with another reference,2 patients in our study experienced fewer emergency room visits and hospital readmissions within 3 months post-infusion compared with 3 months pre-infusion, indicating improved stability with fewer complications compared with the period before treatment.
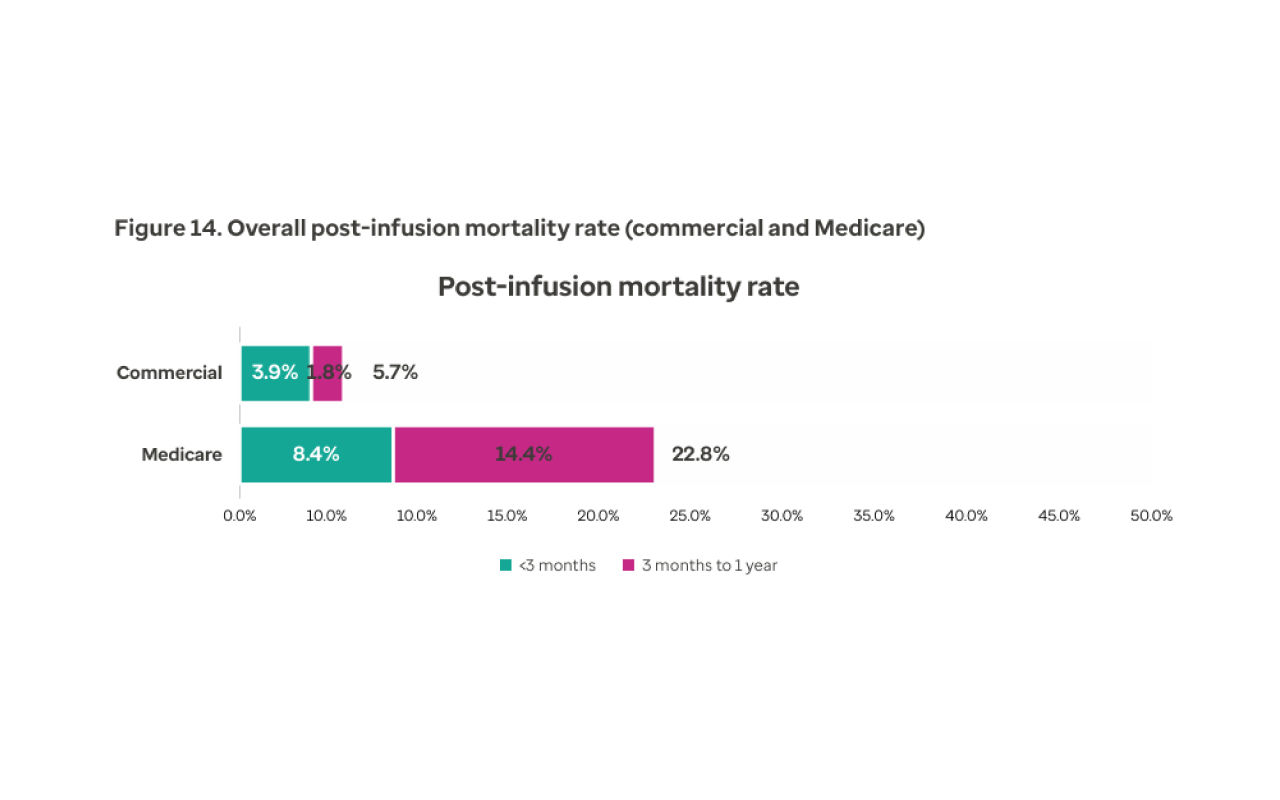
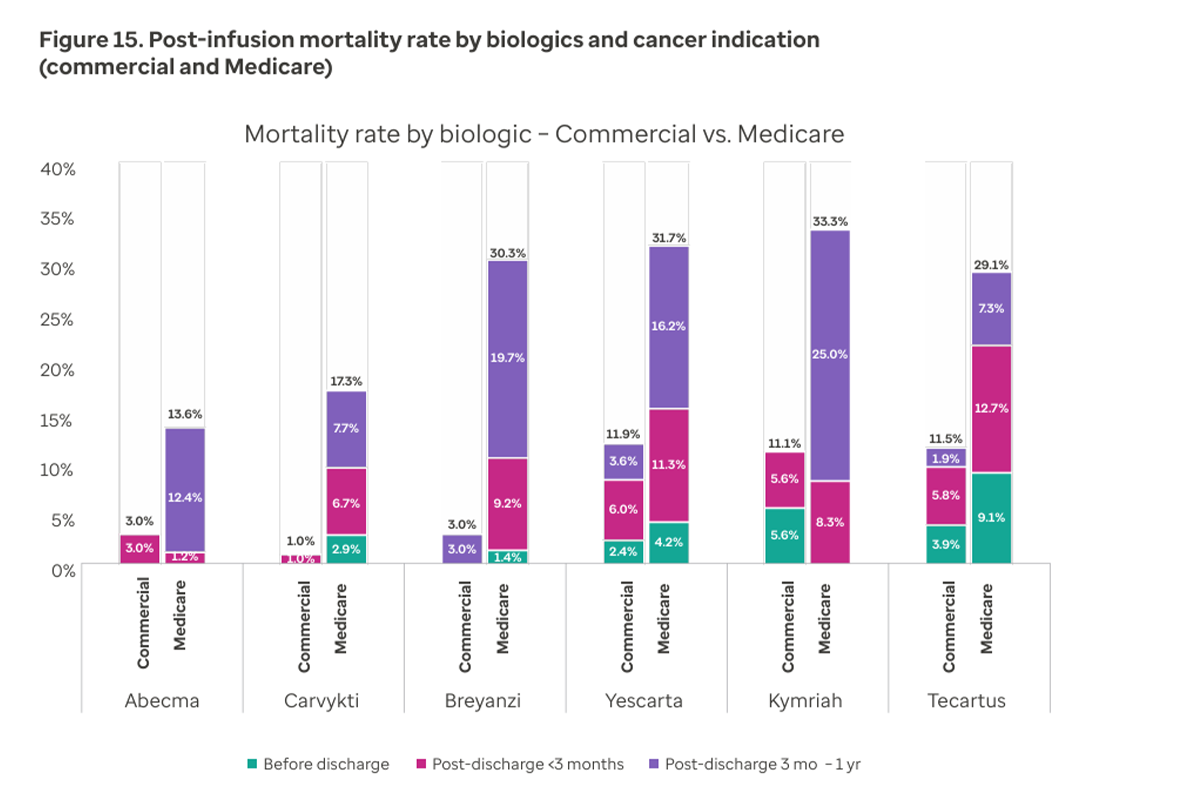
- Mortality rates within 3 months of discharge remained in the single digits — 3.9% for commercial and 8.4% for Medicare populations. These findings indicate that CAR T therapy is generally safe, including for older adults and other higher risk patients.
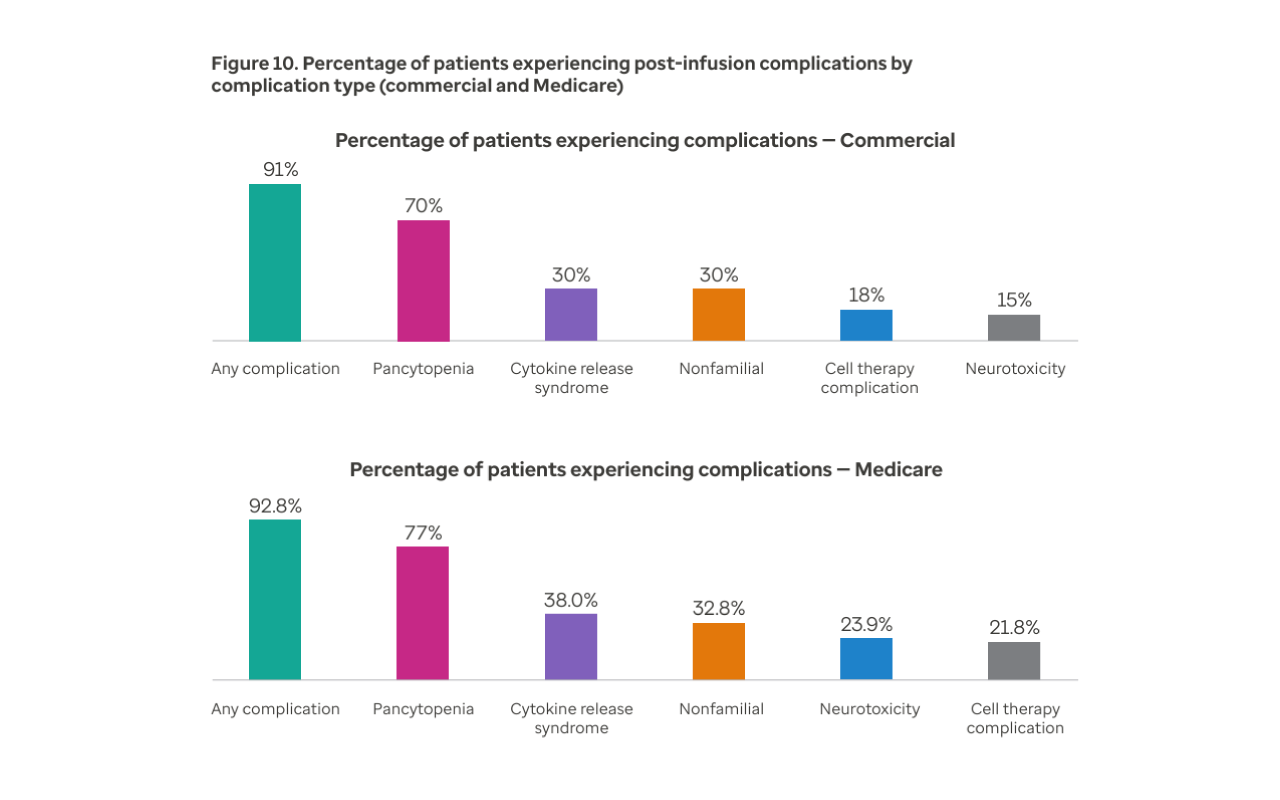
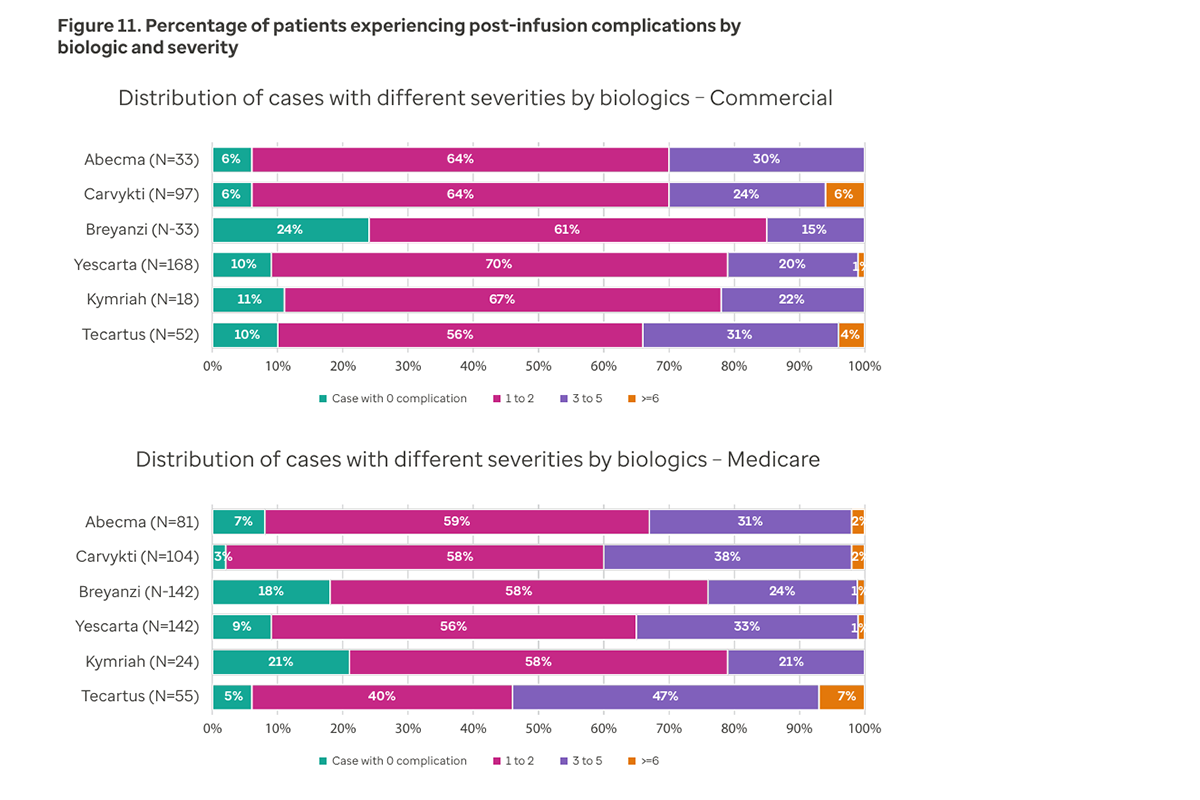
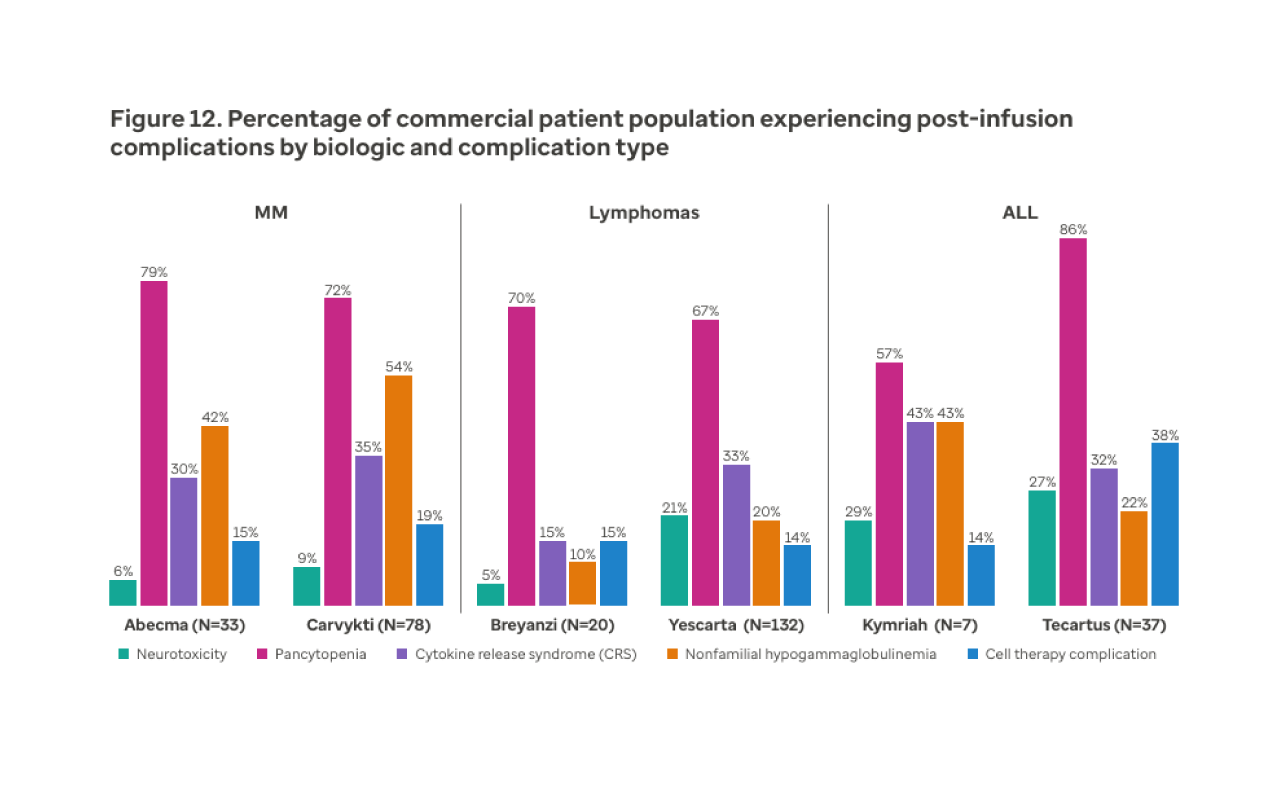
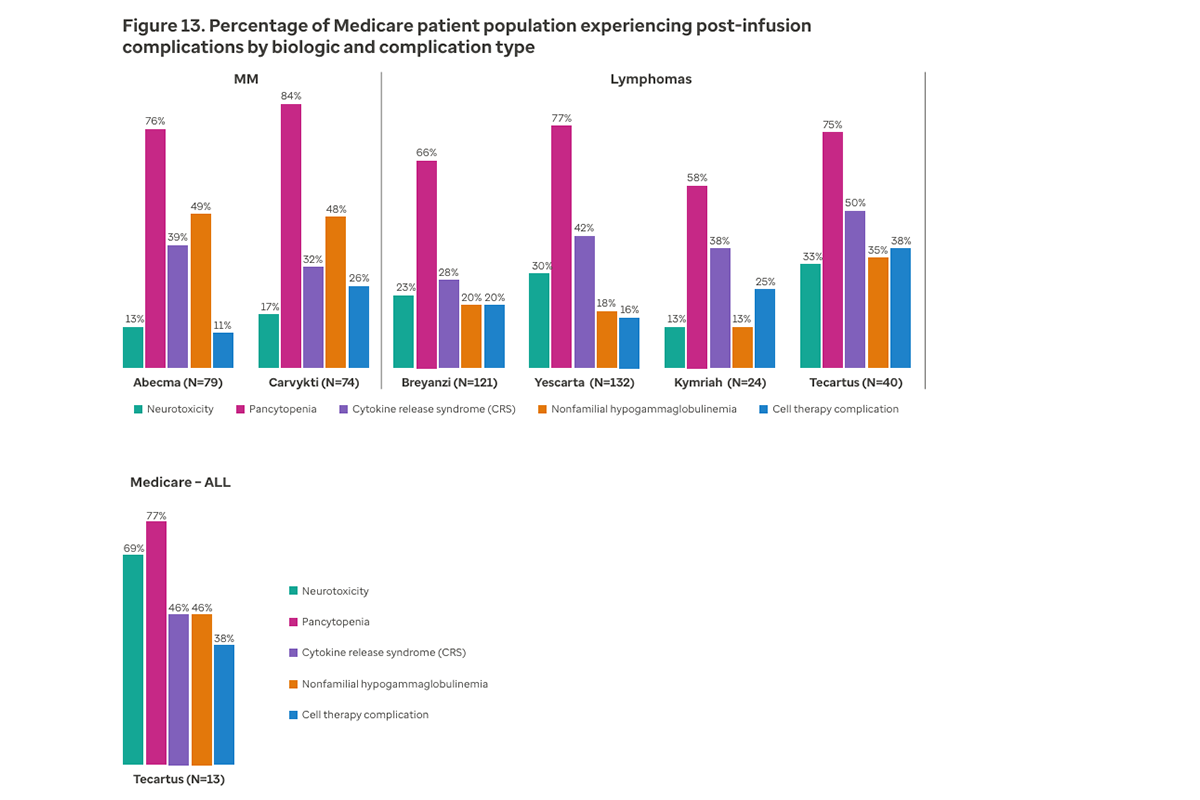
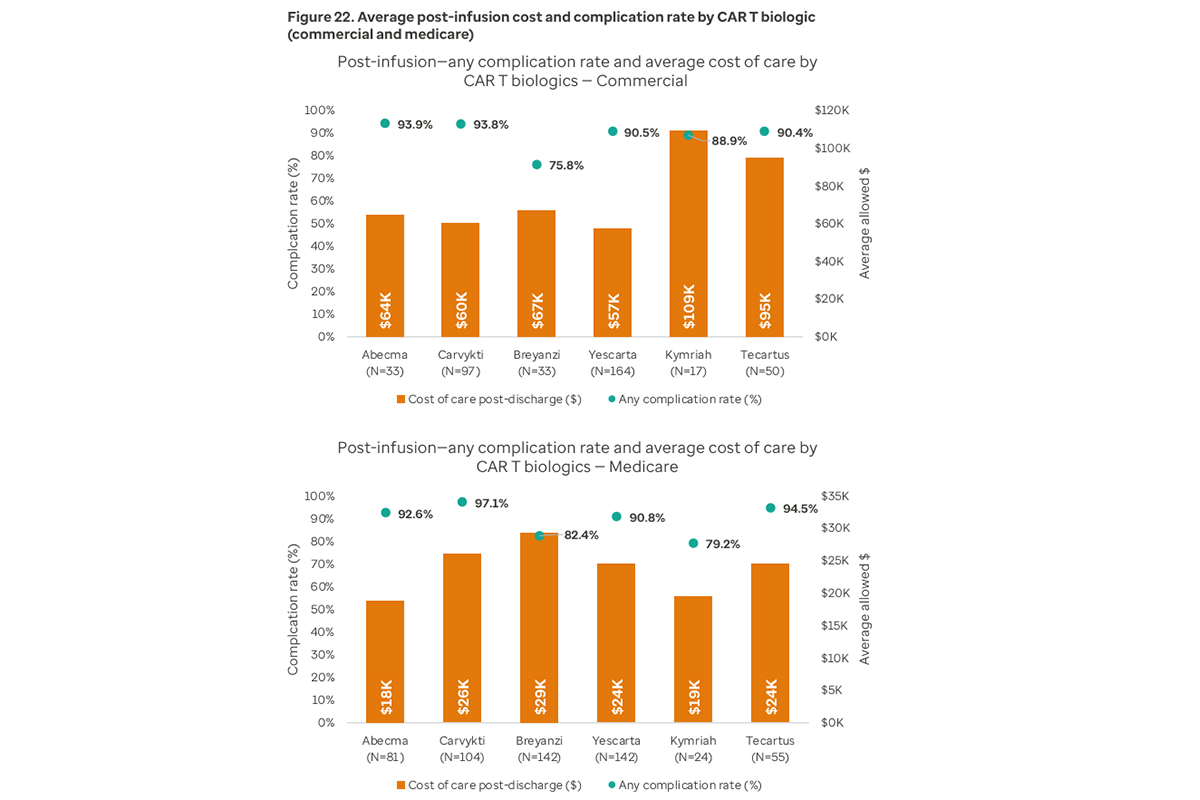
- While most patients experienced at least one complication (most commonly pancytopenia), the majority had fewer than 2 concurrent complications. This demonstrates that, although side effects are common for CAR T therapy, they are generally manageable.
Economic impact
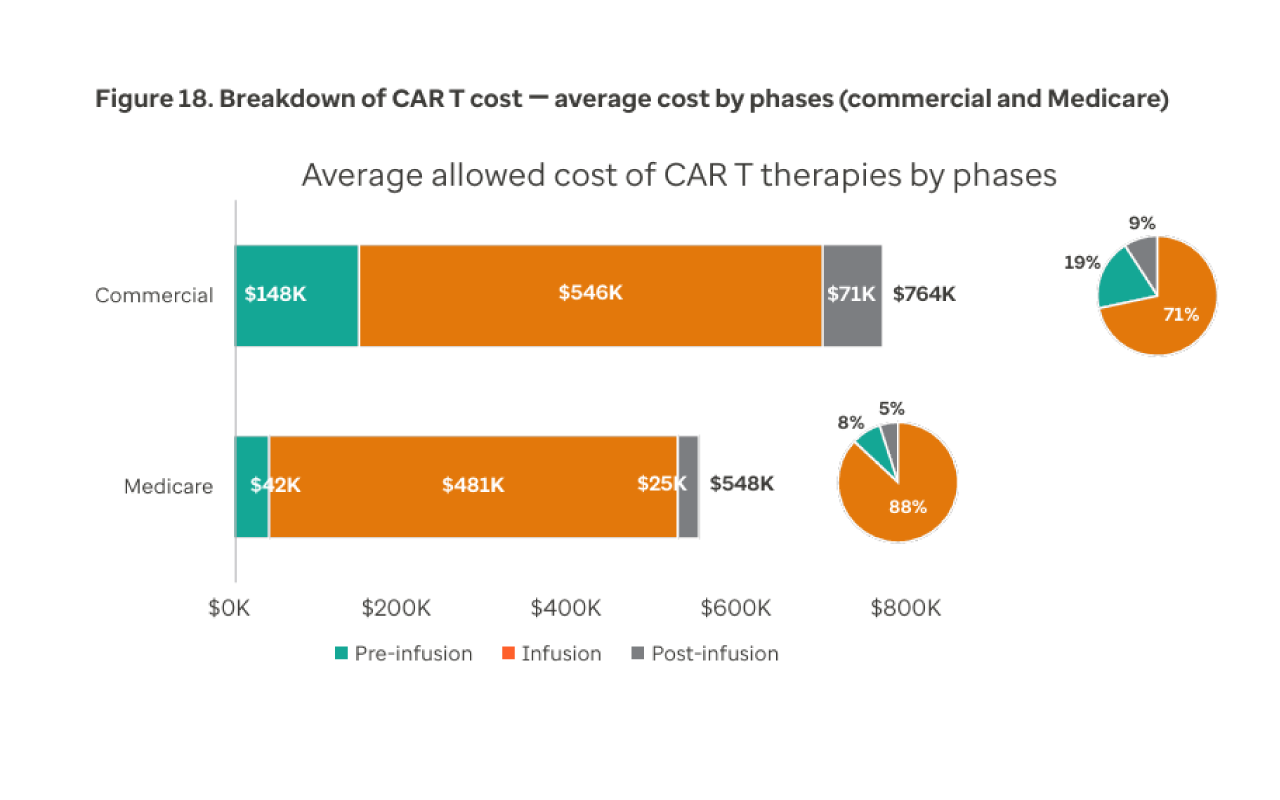
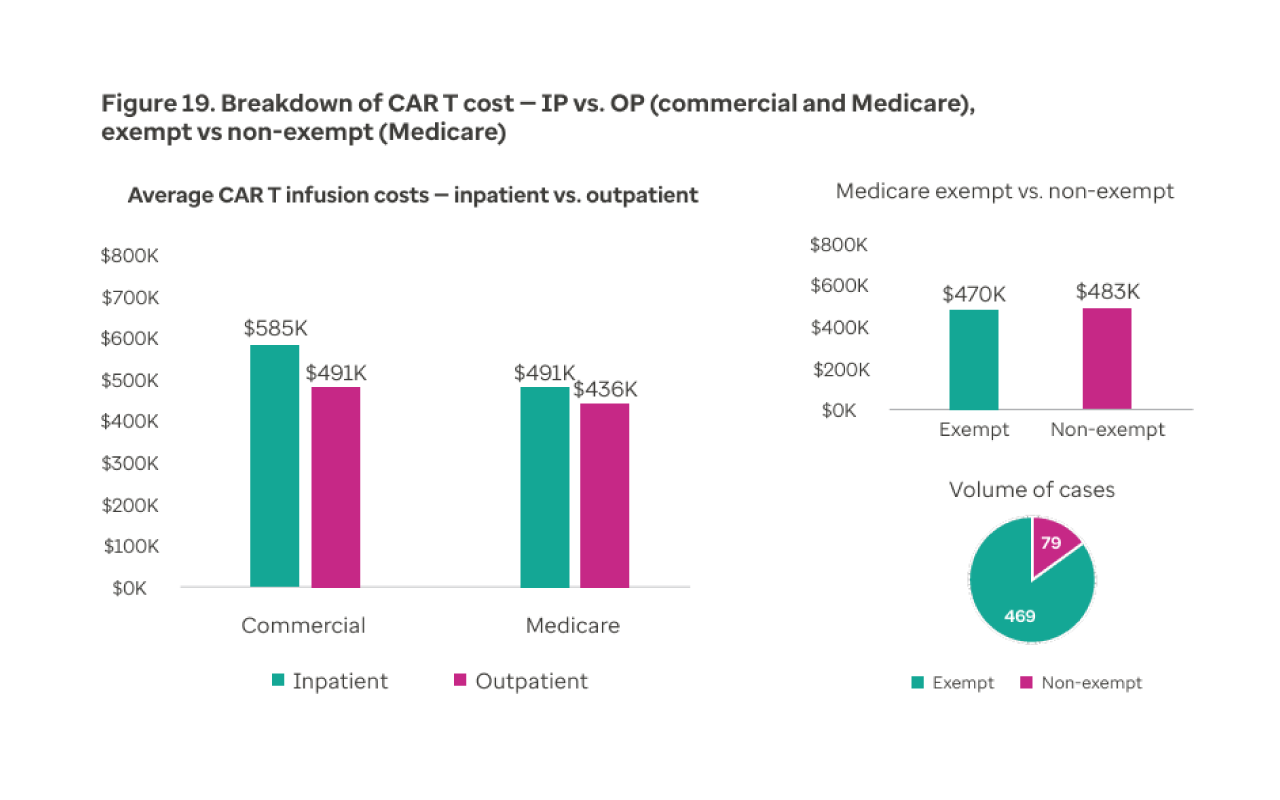
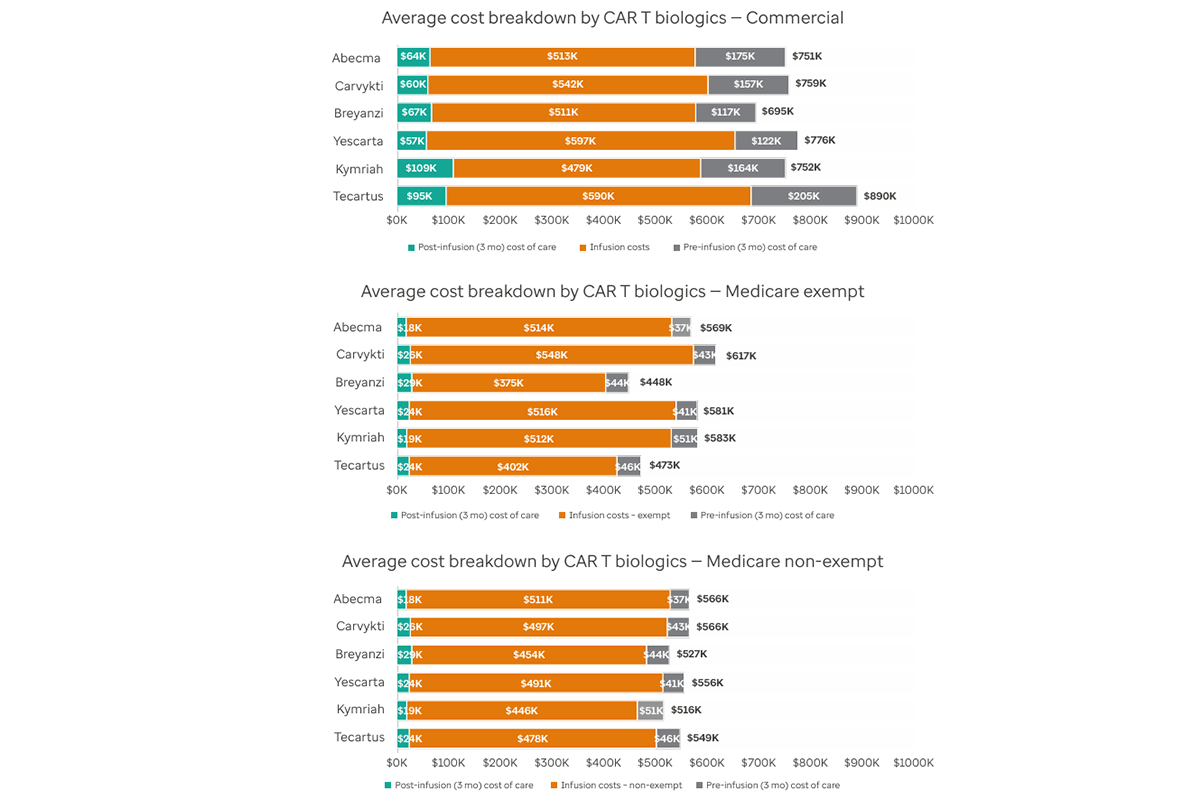
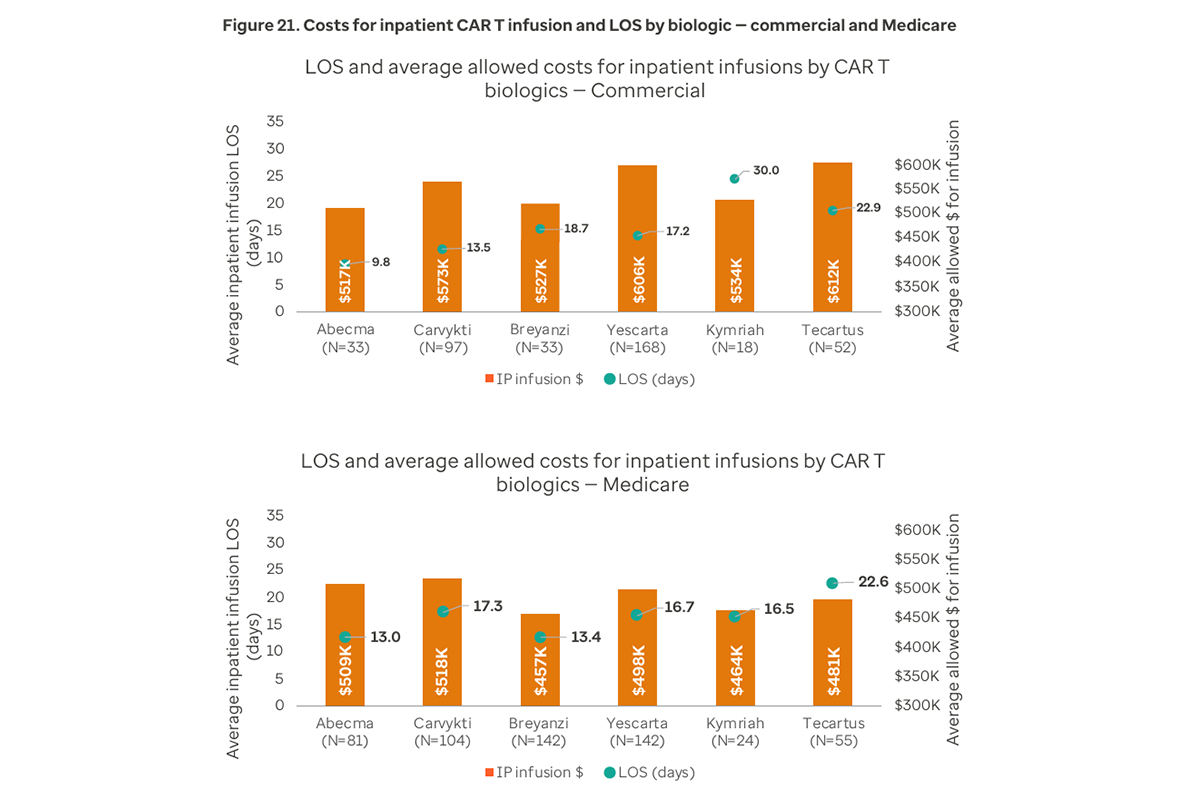
- The average total cost per case for CAR T therapy is $545,528 for the commercial population and $480,676 for the Medicare population. Outpatient infusions are less expensive than inpatient infusions for both the commercial population ($490,723 vs. $585,483) and the Medicare population ($436,066 vs. $490,987).
- Among commercial members, the inpatient readmission rate declined by 10 percentage points 3 months post infusion as compared with the pre infusion period.
- The mean inpatient length of stay (LOS) is 17.3 days for the commercial population and 16.1 days for the Medicare population, with no clear correlation between LOS and cost.
- Post-infusion costs are lower for Medicare ($24,801) than commercial ($70,728). Complication rates are high but do not directly correlate with post-infusion costs.5